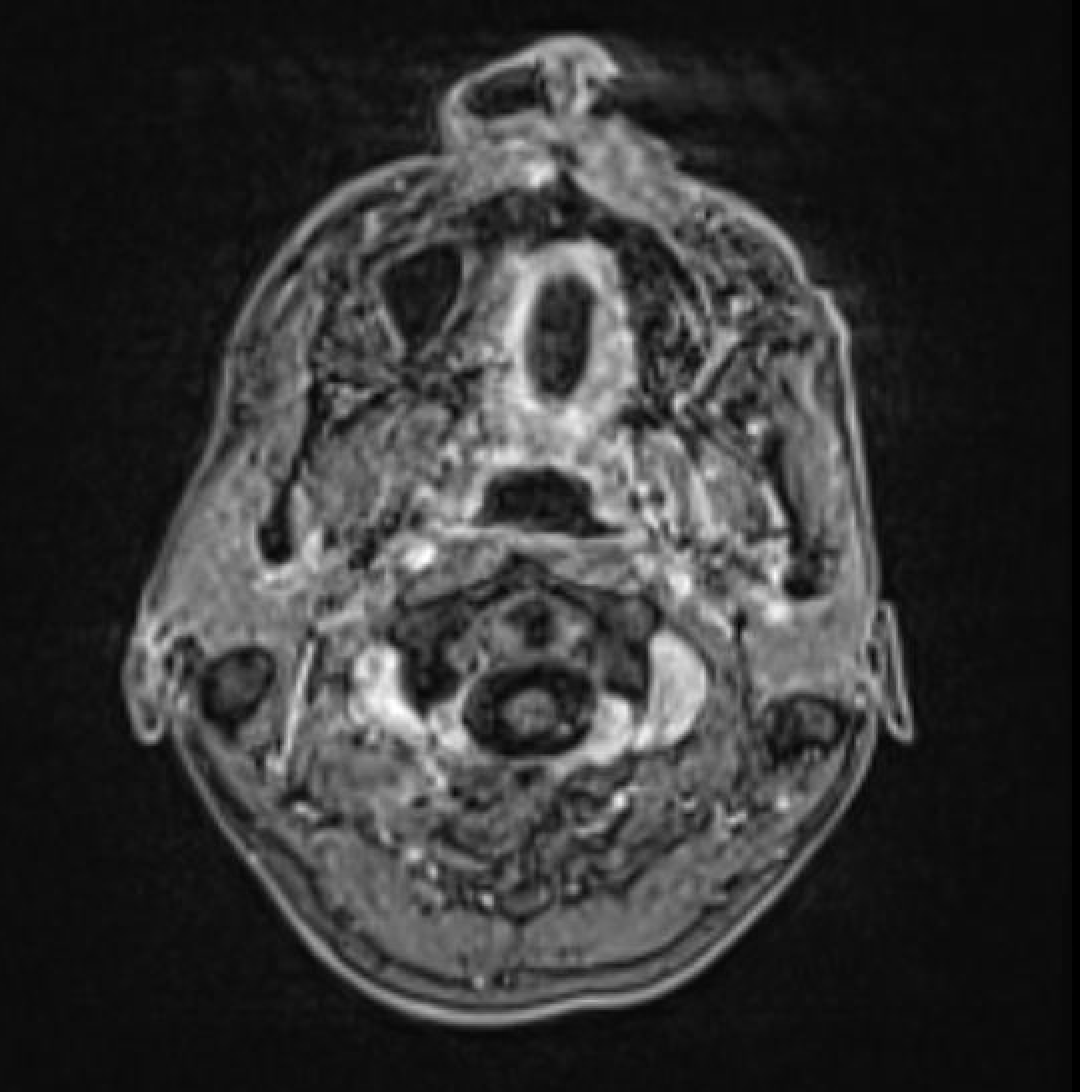
Case Presentation: A 32-year-old man with AIDS (CD4 count 45) presented to the emergency department for altered mental status. More specifically, he reported 5 days of severe bitemporal headache, fatigue, memory disturbance, blurry vision, dizziness, and subjective fevers. His review of systems was also positive for acute-on-chronic diarrhea and a diffuse rash. Given his diagnosis of AIDS, a broad differential was entertained, including infectious, inflammatory, and neoplastic processes. Head CT was abnormal and a follow-up MRI revealed multifocal areas of likely leptomeningeal enhancement. A subsequent lumbar puncture revealed elevated protein and the presence of CMV DNA. Serum CMV DNA quantitative PCR was also detected. He was ultimately diagnosed with disseminated CMV infection.Importantly, he was hospitalized a few weeks prior to this event due to concern for cellulitis in the lower extremity. He had no neurologic signs or symptoms at that time. Dermatology was consulted due to the presence of diffuse hyperpigmented papules and plaques across the face, trunk, and extremities. Punch biopsy of the left upper arm displayed CMV-positive cells with overlying ulceration, consistent with cutaneous CMV infection. This had resulted after hospital discharge and had not clearly been addressed prior to readmission.
Discussion: Cytomegalovirus (CMV) is a prevalent viral pathogen known for precipitating diverse complications in individuals with compromised immune systems, particularly those affected by HIV/AIDS (1). CMV with primary manifestation in the skin is an infrequent occurrence. A limited number of documented cases exhibit similarities with this particular scenario (2, 3). What makes this case particularly intriguing is the notable temporal gap observed between the emergence of cutaneous manifestations and subsequent organ involvement. To the best of our knowledge, there are no other reported cases in the literature where skin lesions served as such an early and distinctive indicator of impending disseminated disease.
Conclusions: After initiating IV ganciclovir, the patient experienced a near resolution of diarrhea, vision changes, and encephalopathy within several days. Only a mild residual headache persisted. This case study underscores the significance of prompt recognition and treatment of disseminated CMV, given its potential impact on several organ systems. Notably, the skin can serve as an early indicator of CMV infection, even preceding symptomatic involvement of other organs by weeks. Given the non-specific appearance of cutaneous CMV, the necessity of a skin biopsy becomes evident for achieving a definitive diagnosis. This interconnected understanding reinforces the critical need for a multidisciplinary approach to the diagnosis and management of disseminated CMV and highlights the importance of considering CMV on the differential diagnosis for immunocompromised patients with cutaneous lesions.