
Background:
Hand‐carried ultrasound echocardiography (HCUE) rivals the image quality and advanced capabilities of standard echocardiography (SE) but offers more portability at less cost. Though not a substitute for comprehensive SE when needed, focused HCUE can supplement cardiac exams and has the potential to help nonechocardiographers answer well‐defined questions at patients' bedsides in under 15 minutes. Yet little has been written on the performance of this test by hospitalists.
Methods:
The 8 participating hospitalists were board‐certified internists with no previous formal training in echocardiography. Training lasted 30 hours and was limited to acquisition and interpretation of 2‐dimensional grayscale and color Doppler images for 6 cardiac assessments: left ventricular (LV) systolic dysfunction, severe mitral valve regurgitation, moderate or severe left atrium (LA) enlargement, moderate or severe LV hypertrophy, medium or large pericardial effusion, and dilatation of the inferior vena cava. The instructor was a hospitalist who had earlier completed a 5‐week course in HCUE. After completion of training, hospitalists performed HCUE on adult inpatients who were referred for SE on weekdays. HCUE was compared to SE performed by echocardiographic technicians and interpreted by attending physician cardiologists who were masked to the HCUE results. HCUE results were analyzed both as dichotomous (positive or negative) and nondichotomous ordinal values (eg, extreme, borderline, negative).
Results:
A total of 314 patients underwent both SE and HCU within a median time of 2.8 hours (25th‐75th percentiles, 1.4‐5. hours). Indeterminate results occurred in only 2% to 6% of the HCUE assessments, despite a high prevalence of obesi (47%) and chronic obstructive pulmonary disease (15%), 2 co ditions known to degrade echocardiographic windows. The pr portional areas under the receiver operator characteristic (RO curves for nondichotomous HCUE results were at least 0.9 for 4 of the 6 abnormalities (Fig. 1). The most common indic tion for SE was assessment of LV function (85%). Whe HCUE results for LV function were analyzed as dichotomou with indeterminate results considered positive, the positive an negative likelihood ratios for HCUE as a test for LV systol dysfunction were 6.9 (95% CI 4.9‐9.8) and 0.2 (95% CI 0. 0.3), respectively.
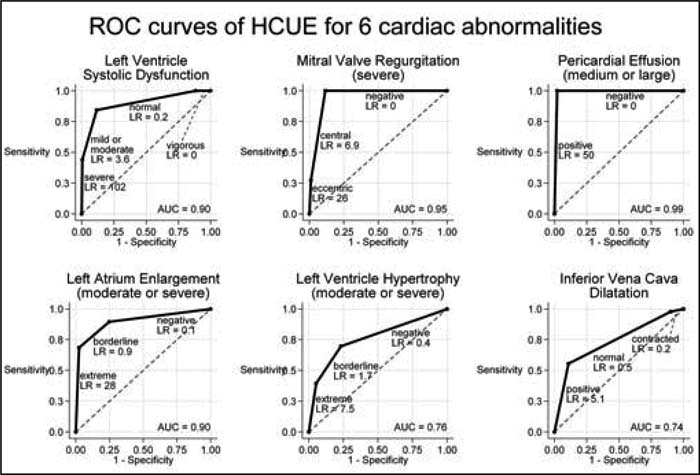
Figure 1.
Conclusions:
The accuracy of HCUE performed by hospitalists after a brief training program was excellent for detection of LV systolic dysfunction, severe mitral valve regurgitation, moderate or severe LA enlargement, and medium or large pericardial effusions. Further research should study the impact of HCUE by hospitalists on patient outcomes.
Author Disclosure:
B. Lucas, none; C. Candotti, none; B. Margeta, none; B. Mba, none; J. Baru, none; J. Asbury, none; A. Asmar, none; R. Kumapley, none; M. Patel, none; S. Borkowsky, none.