Background: Constipation accounts for approximately 20,000 hospitalizations in the United States per year and contributes to increased length of stay for patients hospitalized with other diagnoses. Docusate is routinely prescribed for inpatient constipation although extensive studies have shown minimal effectiveness. It contributes to increased pill burden and polypharmacy for patients, and adds to unnecessary use of resources. At Mount Sinai Hospital, approximately 172,000 doses of docusate are administered per year which translates to 2150 hours of nursing time.
Purpose: We developed a multi-disciplinary, multi-faceted quality improvement project with the goal to decrease the docusate pills ordered by the hospitalist service for the treatment and prevention of constipation by 30%.
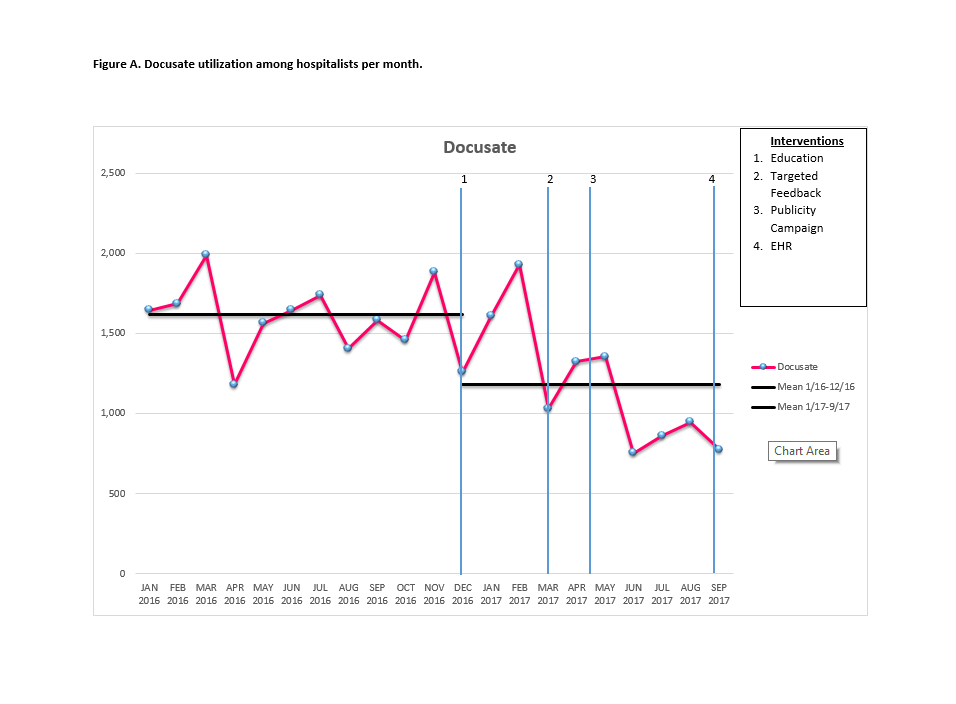
Description: The Student High Value Care team developed this quality improvement project at Mount Sinai Hospital, an urban, tertiary academic hospital. We implemented a robust intervention process involving multidisciplinary staff. The first intervention was an educational presentation to hospitalists, advanced practitioners, and medicine housestaff about the problem of inpatient constipation, evidence on ineffectiveness of docusate, and consequences of overuse. Next, targeted feedback was given to clinicians ordering docusate via email and in person. Third, a local publicity campaign was initiated, placing signs and posters in clinician work areas with the use of slogans, such as “D/C the Docusate.” References to effective alternative medications were provided, along with an inpatient constipation treatment pathway. Finally, the electronic health record (EHR) order was modified by removing docusate from the medicine admission order set. A run chart showing utilization by Hospitalist teams per month is displayed in Figure A.
Conclusions: Through multi-faceted interventions, a successful 31% reduction was achieved over a 10-month period on all hospitalist patients. There is continued reduction reflected by the most recent data, and further reduction is anticipated given the recent final intervention to the EHR. Future changes to the EHR, including advisory warning in the order and removal from other departmental order sets, will result in further reduction. Additionally, with other hospitals in the health system adoption of the same EHR, we expect to see similar reduction throughout other hospitals. Despite discussions with administration, this medication remains on formulary, given the extensive use and patient/provider preference. This project can serve as a model for many other institutions who wish to reduce this unnecessary medication under the similar circumstances. Further studies of de-implementation are needed to effectively reduce this unnecessary medication.