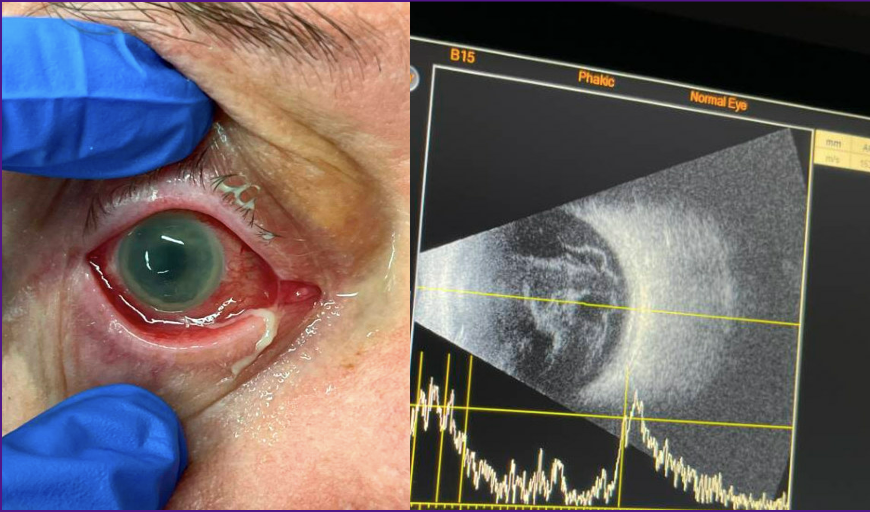
Case Presentation: A 71-year-old man with a history of poorly controlled type 2 diabetes mellitus (complicated by polyneuropathy and diabetic nephropathy), chronic kidney disease, hypertension, hyperlipidemia, and prior left nephrectomy for trauma presented to the emergency department with acute right eye pain, right-sided headache, and sudden vision loss. Two weeks prior, he experienced occipital headaches, intermittent hearing loss, and vertigo. The patient had multiple outpatient visits for persistent headaches and vertigo, and an ophthalmology evaluation noting “junk” in the vitreous on B-scan; he was unable to see a retina specialist due to insurance issues. One day before admission, he developed pink then black floaters in the right eye, followed by complete vision loss and severe pain, prompting ED presentation. Ophthalmology was consulted and suspected endophthalmitis. On admission, the patient was febrile, encephalopathic, and hypoxemic, with acute kidney injury on chronic kidney disease. Ophthalmology performed a vitreous tap, and eye cultures grew hypervirulent Klebsiella Pneumonia. Abdominal imaging revealed a new segment 7 hepatic lesion, likely an abscess. Blood cultures grew Klebsiella pneumoniae. Interventional radiology drained the hepatic abscess, which was also growing Klebsiella Pneumonia.Despite systemic ceftriaxone and repeat intravitreal antibiotics, the patient’s right eye pain persisted, and vision did not improve. Ophthalmology eventually recommended evisceration with tarsorrhaphy of the right globe.
Discussion: This case highlights endogenous endophthalmitis as a rare but devastating complication of hypervirulent Klebsiella pneumoniae (HvKP) liver abscess, a syndrome increasingly recognized in hospital medicine. Endogenous endophthalmitis arises from hematogenous seeding of the eye, often in the setting of systemic infection, typically resulting from a liver abscess without biliary obstruction. In this patient, poorly controlled diabetes was a major risk factor, which impairs neutrophil function.HvKP is distinguished by its hypermucoviscous phenotype (positive string test), K1/K2 capsular serotypes, and enhanced virulence factors, including rmpA/rmpA2 gene expression and siderophore production. While most Klebsiella infections are healthcare-associated, HvKP is often community-acquired. The syndrome is most prevalent in East Asia but is increasingly reported worldwide.Diagnosis of endogenous endophthalmitis requires a high index of suspicion in patients with systemic infection and acute vision loss. Ocular findings include decreased vision, pain, hypopyon, and vitreous inflammation. Negative intraocular cultures do not exclude the diagnosis. Management includes prompt intravitreal and systemic antibiotics, with vitrectomy considered in severe cases. Visual outcomes are poor, especially with virulent organisms such as K. pneumoniae.
Conclusions: This case underscores the importance of early recognition and multidisciplinary management of endogenous endophthalmitis in hospitalized patients with invasive K. pneumoniae liver abscess, particularly those with diabetes. Hospitalists should maintain vigilance for metastatic complications in patients with hypervirulent K. pneumoniae infection, as delayed diagnosis can result in irreversible vision loss or loss of the eye. Collaboration between medicine, ophthalmology, infectious diseases, and interventional radiology is essential for optimal outcomes.
.png)