Background: Hospitalized patients receive time-limited inpatient care, often from a hospitalist who does not longitudinally manage medications. Hospitalized patients are at risk for medication errors and adverse drug events (ADEs) due to poor medication reconciliation, drug-drug interactions (DDIs) and drug-gene interactions (DGIs) from newly-started medications, and/or lack of communication about changes in therapy. These challenges provide the rationale for establishing a virtual post-hospitalization Personalized Therapeutics Clinic (PTC) to provide specialized prescribing assessment/consultation and patient education. We aimed to identify DDIs and DGIs identified in discharged hospitalized patients at a post-discharge PTC visit.
Methods: Patients identified as high risk for medication-related events were approached for enrollment in the PROTECT-Rx trial (NCT# 05166694) at the University of Chicago and offered a one-time virtual visit at the PTC. Adults were eligible if they were prescribed ≥5 medications and taking ≥1 significant inducer or inhibitor, or if they were taking ≥1 medication with potentially actionable pharmacogenomic (PGx) information. Recruitment occurred through Electric Medical Records (EMR) generated auto-filtered lists, provider referrals, and posted flyers. A dedicated research coordinator approached eligible patients and obtained informed consent. Broad PGx testing was provided at no cost as part of the trial. During the PTC visit, participants met with a clinical pharmacologist who assessed DDIs and DGIs and composed formal recommendations to both patients and their treating providers. All consultations were documented in the EMR. Prescribing patterns and the rates of DDIs and DGIs were assessed at baseline and at 3 months. The primary outcome was the change in the composite rate of DDIs and DGIs from baseline to 3 months.
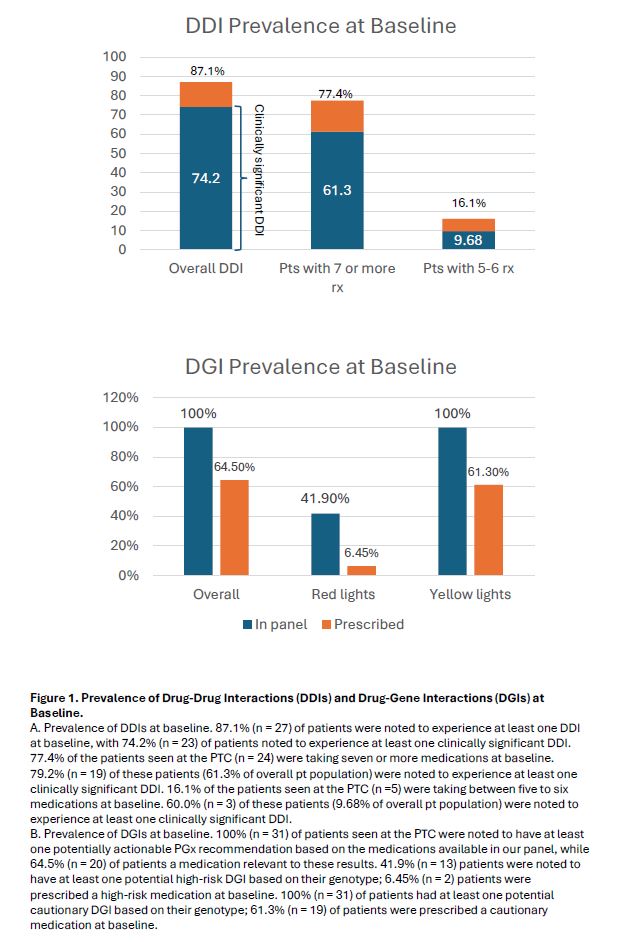
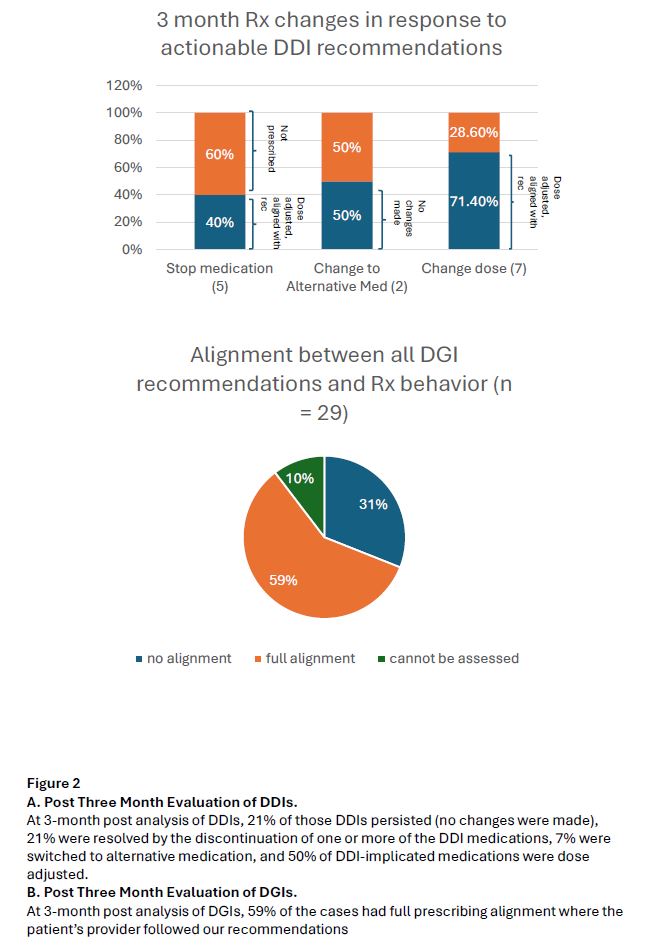
Results: The analysis included 31 patients with a mean age of 53.8 years, 80% were female, and 67.7% were insured through Medicare or Medicaid. The 5 most common medications patients were taking were acetaminophen, pantoprazole, insulin, albuterol, and atorvastatin. The top 5 most encountered medications with actionable PGx information were pantoprazole, atorvastatin, hydrocodone, metoprolol, and amlodipine. At baseline, 74.2% of patients had clinically significant potential DDIs and 64.5% of patients had cautionary/high-risk DGIs. We provided DDI recommendations for 87.1% of patients and DGI recommendations for 67.7% of patients. At 3-month post analysis of DDIs, 21% of those DDIs persisted (no changes were made), 21% were resolved by the discontinuation of one or more of the DDI medications, 7% were switched to alternative medication, and 50% of DDI-implicated medications were dose adjusted by 3 month follow-up. At 3-month post analysis of DGIs, 59% of the cases had full prescribing alignment where the patient’s provider followed our recommendations.
Conclusions: Clinically significant DDIs and DGIs were highly prevalent among hospitalized patients recruited to our study, underscoring the substantial need for specialized medication review in this population. Subsequent changes in prescribing were mediated in a substantial proportion of visits, showing the potential promise of a post-hospitalization PTC visit. These findings deserve formal investigation in a randomized study to determine the impact on mitigating or preventing ADEs.