Background: Academic medical centers (AMCs) increasingly rely on partnerships with affiliated community hospitals (CHs) to expand inpatient capacity by transferring lower-acuity patients. These partnerships are often limited by differences in specialty resources and infrastructure, narrowing the pool of eligible patients for transfer. Understanding the clinical and operational barriers to transfer is essential to guide targeted resource expansion and strengthen network capacity.
Methods: We performed a retrospective analysis of triage hospitalist documentation at a large urban AMC over a 12-month period (July 2023–July 2024). For each Hospital Medicine (HM) admission request from the emergency department, a triage hospitalist assessed the patient’s suitability for admission at the AMC versus transfer to the CH and documented their decision-making using a structured note template. Required fields included: specialty service requirements, patient or family declination, bed unavailability, patient acuity, and staffing restrictions, with an optional a free text space for “other.” We extracted note data from the electronic health record using SQL queries and calculated absolute frequencies for each barrier. Subset analyses were performed for patients without exclusion criteria to identify potentially modifiable factors.
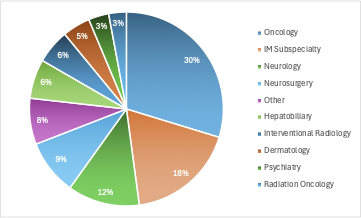
Results: During the study period, 6,217 triage notes were reviewed. Specialty service requirements accounted for 3,349 (53.9%) of all documented transfer barriers (Figure 1), most frequently involved services being oncology, neurology, neurosurgery, hepatobiliary, interventional radiology, and other medicine subspecialties (rheumatology, gastroenterology, hematology and nephrology). Among patients without other specific barriers, 62% declined transfer when offered.
Conclusions: Subspecialty availability, patient assent, and appropriate level-of-care availability were the most common barriers to interhospital transfer. These findings have informed targeted interventions at our institution, including expanding consultant availability at the community hospital and improving consent rates and bed access.