
Background: Hospitalization for alcohol withdrawal syndrome (AWS) is frequent, accounting for over 2 million national admissions annually in the United States.[1, 2] Benzodiazepines remain the guideline-recommended treatment for AWS, yet many hospitals are adopting phenobarbital protocols leading to potentially different practices within hospital emergency departments (EDs), intensive care units (ICUs) and medicine floors.[3, 4] There is a lack of data on how hospitalist and acute medical floors are treating AWS, and what challenges they face with evolving AWS treatment practices. The aim of this study is to describe hospitalists’ current AWS management practices.
Methods: We used a mixed-methods approach with a survey and focus groups. A convenience sample of hospitalists were recruited from a national hospital medicine research network to participate in the study. The survey and focus groups took place virtually. The survey and focus groups included questions exploring local AWS management, practices, and hospitalists’ views on AWS treatment. Survey data was captured using REDCap and summarized using descriptive statistics. Focus groups were digitally recorded, transcribed and analyzed using thematic analysis.
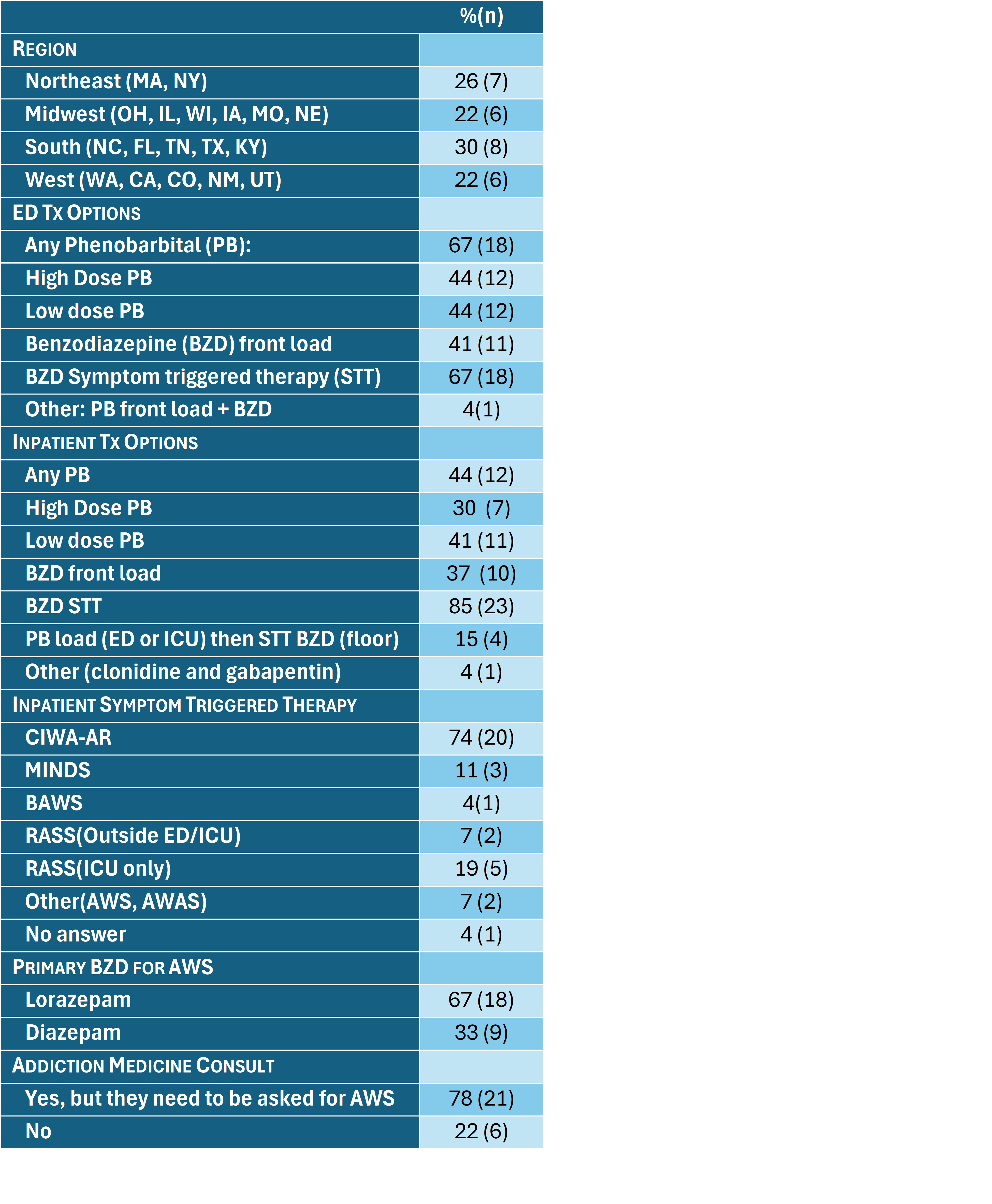
Results: A total of 33 hospitalists representing 27 hospital systems participated in this study. The hospitalists participating were from hospitals distributed across the Northeast (7), Midwest (6), South (8), and West (6) census districts. Survey results for ED and inpatient phenobarbital protocols, and benzodiazepines protocols are presented in Table 1. Focus-group analysis identified five themes (Table 2): 1) A “wild west” or “vibes based approach” to AWS therapy selection, 2) High variation in AWS treatments within hospital units (ED/floor/ICU) and between clinicians, 3) A desire for more research to guide practice, 4) Outcomes of interest for AWS are primarily focused on logistics of care, and secondarily in AWS complications and long-term alcohol use disorder treatment outcomes, 5) Shared-decision making with patients for AWS treatment is rare and often limited due to patient impairment.
Conclusions: Hospitalists in our study reported that benzodiazepines were the most common AWS treatment on the acute medical floor, but phenobarbital was increasingly available and being used either in the ED or the ICU. We found floor services had limited phenobarbital options, and providers were left to determine the course. More research is needed to determine the best therapy for AWS, and to support an evidence-based and uniform approach to treatment of AWS for patients across treatment settings.
.png)