
Background: A limited evidence base, vulnerability to opioid-related stigma and racial bias, and healthcare system constraints contribute to suboptimal inpatient care for people with Sickle Cell Disease (SCD). Health care professionals (HCP) are forced to contend with these constraints during inpatient SCD care delivery, which can lead to distress and burnout. Moral distress is a framework that describes the negative emotions felt by HCPs when they are unable to act in a manner that aligns with their ethical values. Our study evaluates the moral distress experienced by HCPs during inpatient care of people with SCD.
Methods: This study is a secondary analysis of a larger qualitative study of ideal care for hospitalized individuals with SCD. We analyzed 22 transcripts from HCPs including physicians, advanced practice providers (APP), nurses, residents, pharmacists, and social workers utilizing the framework of moral distress. The interviews were thematically coded using inductive and deductive reasoning to identify the five types of moral distress defined by Fourie and Morley: constraint, conflict, tension, uncertainty, and dilemma.
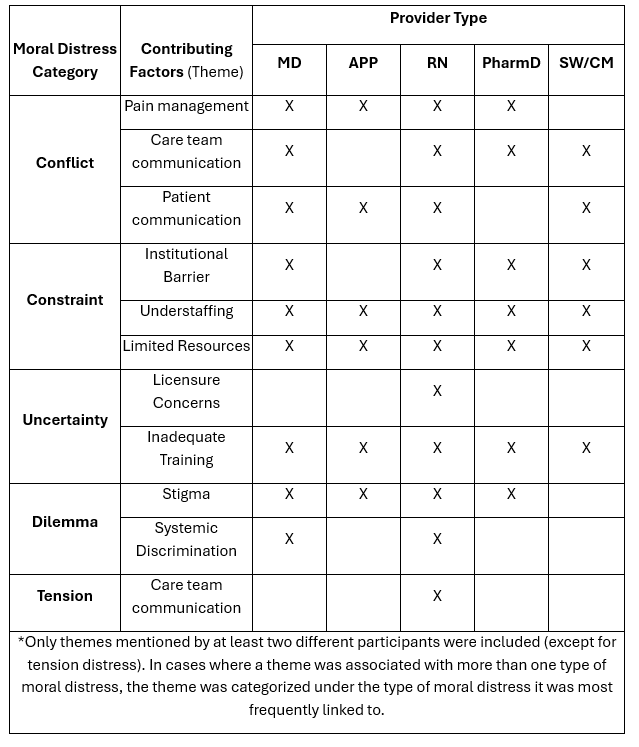
Results: We identified all types of moral distress in the transcripts (Table 1) with illustrative quotes listed in Table 2. Constraint distress, which was expressed by all types of HCPs interviewed, was the most common type of moral distress experienced by HCPs and was linked to institutional barriers including Emergency Room boarding times and understaffing. Conflict and tension distress arose when there were conflicts among team members, often due to disagreement about pain management plans or ineffective communication. Tension distress came up less frequently likely due to the unspoken nature, and that interview questions did not address that particular type of distress. Uncertainty distress was linked to licensure concerns (from nurses due to high dose narcotics), lack of disease-specific education (all HCP types), and lack of clear pain management plans. Dilemma distress emerged when HCPs identified the impacts of systemic discrimination and stigma on the patients for whom they were caring.
Conclusions: Moral distress is experienced by HCPs in their care for individuals with SCD. HCPs cited systemic inequities as well as institutional barriers to providing ideal care. Mitigating these causes of moral distress will require system-level changes and institutional prioritization of hospital care for individuals with SCD through interventions like dedicated units and specialized care teams. Additionally, disease-specific education can be directed towards staff on specific units (if there is a dedicated unit) or can be part of general education to help all HCPs better understand the complex needs of patients with SCD. These same principles can likely be applied to other populations with intersecting and complex needs such as people who are incarcerated, adults with complex congenital conditions, and patients with complications of substance use disorder.
.png)