Background: Effective capacity management of hospitalized patients remains a challenge within many medical institutions. Inpatient flow efficiency is an increasingly critical component of hospital operations, as an increased prevalence of chronic diseases manifests, the aging population continually grows, and we subsequently see a rise in higher acuity disease states that warrant inpatient level of care. The Sg2 (a Vizient, Inc. company) 2024 Impact of Change report projects that, within the U.S., there will be a 3% rise in inpatient discharges and a 9% increase in inpatient days over the next decade [1]. Thus, it is crucial that healthcare systems adopt innovative solutions to meet growing inpatient capacity demands.
Purpose: Multiple studies have demonstrated variances in operational success related to timely discharges and their impact on inpatient flow effectiveness [2-6]. At MD Anderson Cancer Center, increasing inpatient capacity demands created a clear urgency for action. Thus, we strived to implement a multidisciplinary timely discharge program within our complex medical oncology population. Our goal was to uproot systemic bottlenecks that encumber efficient discharge planning, and in turn, improve emergency department boarding times and ultimately hospital compression.
Description: We utilized the cyclic Plan-Do-Study-Act (PDSA) method to engage stakeholders and identify systemic barriers that contributed to delays in timely patient discharge. This process facilitated the development of the DiCE (Discharge-barrier identification, Communication, Escalation) model, a novel infrastructure that was imperative in the success of our timely discharge program (Figure 1). We deployed this model within our medical oncology pilot units at the start of July 2024, in collaboration with multi-disciplinary teams to alleviate discharge barriers. Key Performance Indicators (KPIs) to evaluate program outcomes were as follows: 1) Increase rates of 9 AM discharge order entry to >50% 2) Increase rates of discharge by noon to >50% 3) Increase Estimated Discharge Date (EDD) accuracy 1-day prior to discharge to >50%
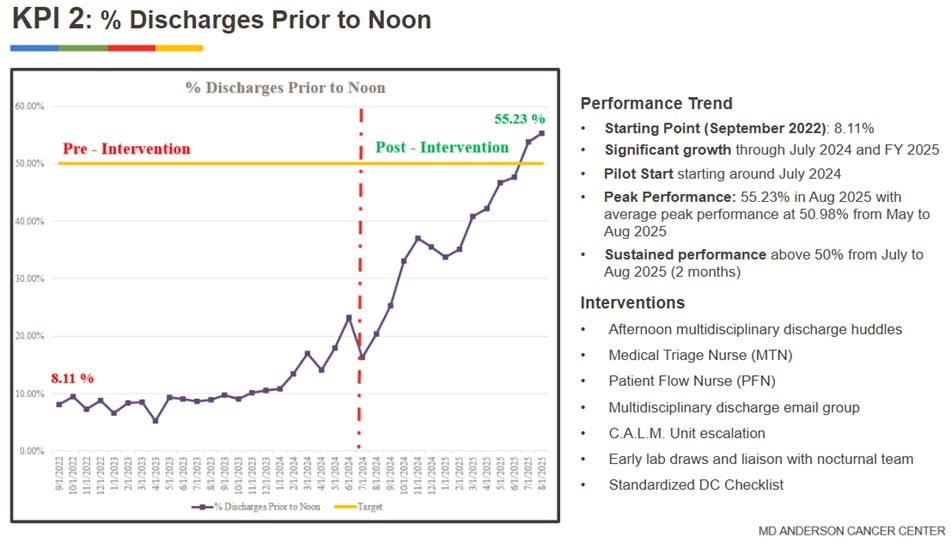
Conclusions: Implementation of a novel and comprehensive timely discharge program significantly improved discharge efficiency in a complex medical oncology population. EDD accuracy 1-day prior to discharge increased from 42.28% to 54.12% post-intervention. Discharge orders entered by 9 AM increased dramatically from 7.52% in September 2022 to 53.87% by August 2025, paralleled by an increase in patient discharges by noon from 8.11% to 55.23% over the same time frame (Figure 2). We anchor the success of our initiative to the creation of a process for proactive identification of systemic discharge barriers and early escalations to resolution. The DiCE model for timely discharges is rooted in the power of a closed-loop communication process. This approach reduced emergency department boarding times from 5-6 hours to 2-3 hours, expediting time-sensitive treatments, enhancing multi-disciplinary care coordination, improving patient flow and alleviating overall hospital compression.
.png)