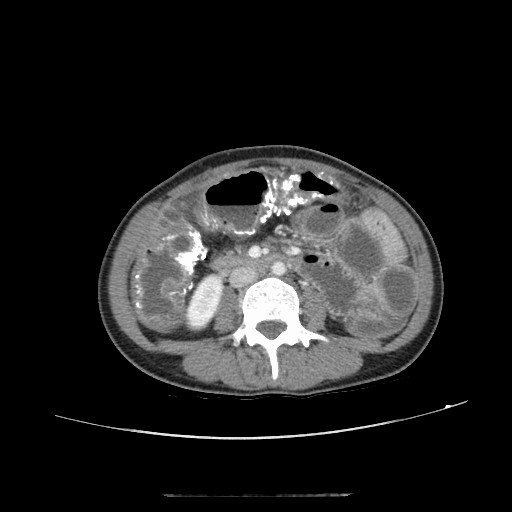
Case Presentation: A 32-year-old woman with no prior medical history presented with 3 days of severe diffuse abdominal pain, nausea, vomiting, obstipation, and abdominal distention. She reported no flatus and had recently started drinking a complex herbal tea mixture (>25 herbs) for constipation and improving energy. For over 10 years, she intermittently used unnamed herbal remedies for weight gain, discontinued recently due to vague symptoms. On exam, vital signs normal. Pertinent labs: Na 134 meq/L, Cl 95 meq/L, total bilirubin 1.5 mg/dL. Lactate negative. CBC normal. CT abdomen/pelvis revealed serpiginous metallic density in the ascending, hepatic flexure, and transverse colon, small bowel obstruction, and thickened colonic wall-suggesting of idiopathic mesenteric phlebosclerosis (IMP) with possible venous ischemia. She received IV fluids and empirical antibiotics. Due to worsening symptoms, she underwent diagnostic laparoscopy, which revealed severely diseased, blackened colon with abscesses. An open right colectomy with end ileostomy and a mucus fistula was performed. She recovered well and was discharged with surgical follow-up.
Discussion: IMP is a rare, non-thrombotic ischemic colitis characterized by calcification and sclerosis of mesenteric veins. It is strongly linked to long-term herbal medicine use. It predominantly impacts Asian populations, with an occurrence ~ 0.01 per 100,000 individuals in Japan. While poorly understood, chronic ingestion of certain herbal toxins likely induces venous fibrosis and obstruction. IMP symptoms are non-specific (abdominal pain, diarrhea, vomiting, obstruction), and reported 10-20% early cases have no symptoms which makes diagnosis challenging. CT is the preferred modality for diagnosis, often revealing characteristic serpentine, thread-like structures along the colon frame caused by calcified mesenteric veins, in over 90% cases. Colonoscopies are safe, and reveals typical dark purple or brown mucosa. Confirmation of diagnosis relies pathologic findings of the hallmark of chronic ischemic colitis caused by fibrosis, thickening, calcifications/sclerosis, and circumferential stenosis of venous walls. Management is usually conservative by discontinuing herbal intake and bowel rest, which is effective and in up to 90% of patients. Limited reports suggest aspirin, anticoagulants, and mesalazine may be effective in some cases. Surgical resection is reserved for patients with severe complications such as persistent symptoms, recurrent intestinal obstruction, massive hemorrhage, ischemia or perforation-as in our patient. This case underscores the catastrophic potential of chronic herbal ingestion, culminating in rare pathology requiring major surgery. The CT finding of metallic density is highly suggestive of the offending agents.
Conclusions: IMP is a diagnostic challenge due to non-specific presentation and lack of serum markers. It should be considered in Asian patients with refractory abdominal pain or small bowel obstruction, especially those with a history of long-term complex herbal use. Early identification via imaging may allow for successful conservative management. Hospitalists must be aware of this diagnosis, as it underscores the importance of a detailed medication history including all herbal supplements and the potential for these products to cause severe, life-threatening gastrointestinal pathology.