Background: Many patients are discharged from the hospital to post-acute rehab in a skilled nursing facility (SNF). These care transitions can be error-prone, hampered by inadequate patient preparation for rehabilitation and insufficient communication between care providers. The readmission rate from SNF was 23.5% in 2006, costing Medicare $4.34 billion. Prior studies show 30% of these readmissions are potentially avoidable. Our HOPE consultation program was designed to optimize the transition from hospital to SNF via an inpatient consultation and a post-discharge in-facility follow-up by an Advanced Practice Provider (APP) with geriatrics attending supervision.
Methods: Patients age 55 and older, discharged from the hospital to post-acute care rehab in a skilled nursing facility (SNF) were eligible for a HOPE consultation. An experienced geriatrics nurse practitioner evaluated each inpatient HOPE patient with the goal of identifying and treating geriatric syndromes, setting appropriate expectations for SNF care with patients/care givers, assessing rehabilitation potential, initiating discussion on contingency plans if rehab goals are unmet, and discussing goals of care. Consultation recommendations were communicated to the primary team and incorporated into discharge planning prior to patient discharge. Post-discharge follow-up within 1 week was conducted by the APP via a phone call or more often, a visit to the SNF. During this follow-up an APP reviewed and discussed high risk/new medications, rehabilitation participation, and appointments/labs/hospital recommendations with SNF medical staff. The study compared readmission rates for all Medicine/Surgery patients in our hospital with and without HOPE consultation who were 55 years or older and discharged to SNF between August 2016 – August 2017.
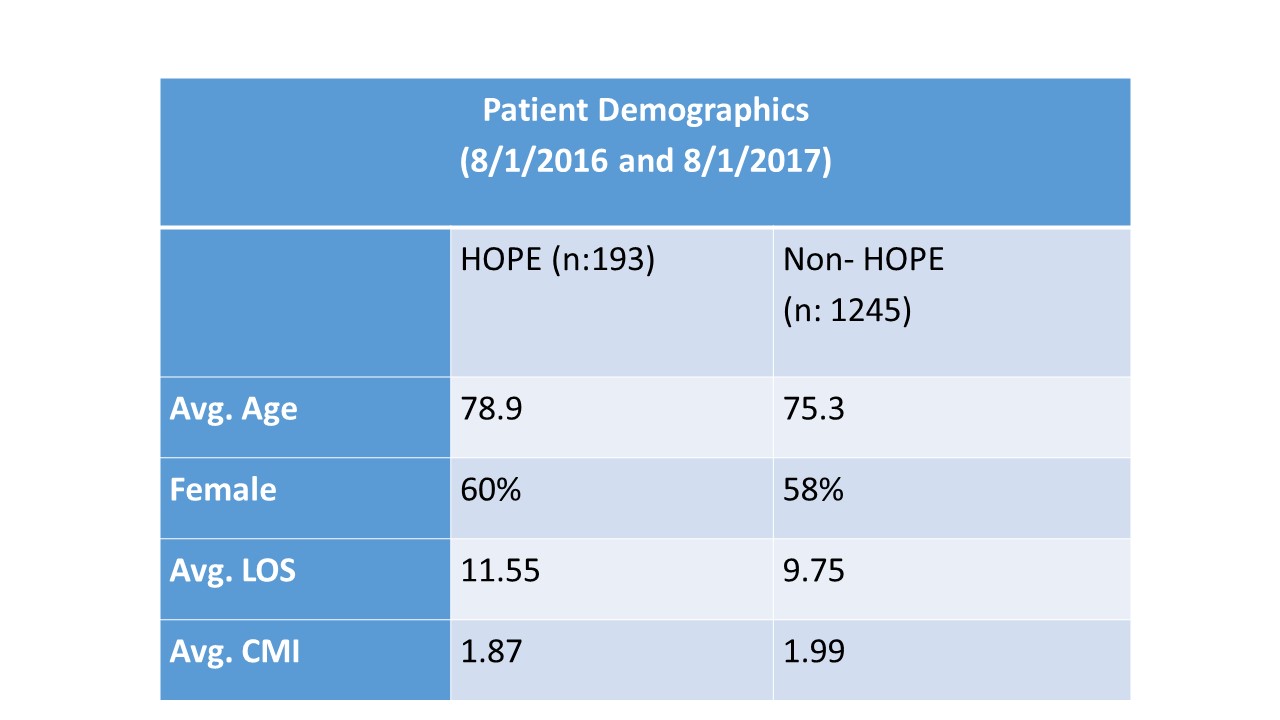
Results: A total of 1,245 non–HOPE and 193 HOPE patients were analyzed. The 7, 14, and 30-day readmission rates for HOPE patients were 5.9%, 8.6%, and 12.8% respectively, compared to 5.4%, 10.9%, and 19.3% in the comparison group. There was a statistically significant 33% reduction in the 30-day readmission rate despite older age and longer hospital stay in the HOPE group. The HOPE APP identified errors or near misses in 7% of patients during SNF follow-up and made non-medication and/or medication recommendations in 80% of SNF HOPE encounters.
Conclusions: A longitudinal, dual-consultation service model with a paired consultation in-hospital, and in-SNF is an effective means of improving care transitions in higher risk older adults. This model provides opportunity for improved communication, identification of errors during care transitions, and reduction in preventable readmissions.