Background: Common hospitalist workflow includes hospitalists balancing inpatient care and discharges with new Emergency Department (ED) admissions. This model can strain hospitalist efficiency. We hence introduced a Double ED Admitter (DEDA) Model, where we designated two hospitalist physicians exclusively for ED admissions during peak hours, allowing rounding hospitalists to focus on inpatient care and timely discharges. We evaluated the impact of this intervention on hospitalist and ED performance metrics.
Purpose: We conducted a retrospective analysis of hospital throughput metrics before and after implementation of the DEDA model at INTEGRIS Health Baptist Medical Center which is a tertiary care hospital in Oklahoma City. We evaluated the following metrics: Length of Stay (LOS), LOS Observed/Expected (O/E) ratio, Geometric mean LOS (GMLOS), percentage discharges by noon, and mean monthly discharges for hospitalist patients. For ED metrics, we evaluated the percentage of patients staying in the ED longer than 120 and 280 minutes after an admit order, mean time from admission order to ED departure, and mean total ED LOS for admitted patients. We used SPSS software to perform descriptive statistics. A p-value < 0.05 was considered statistically significant
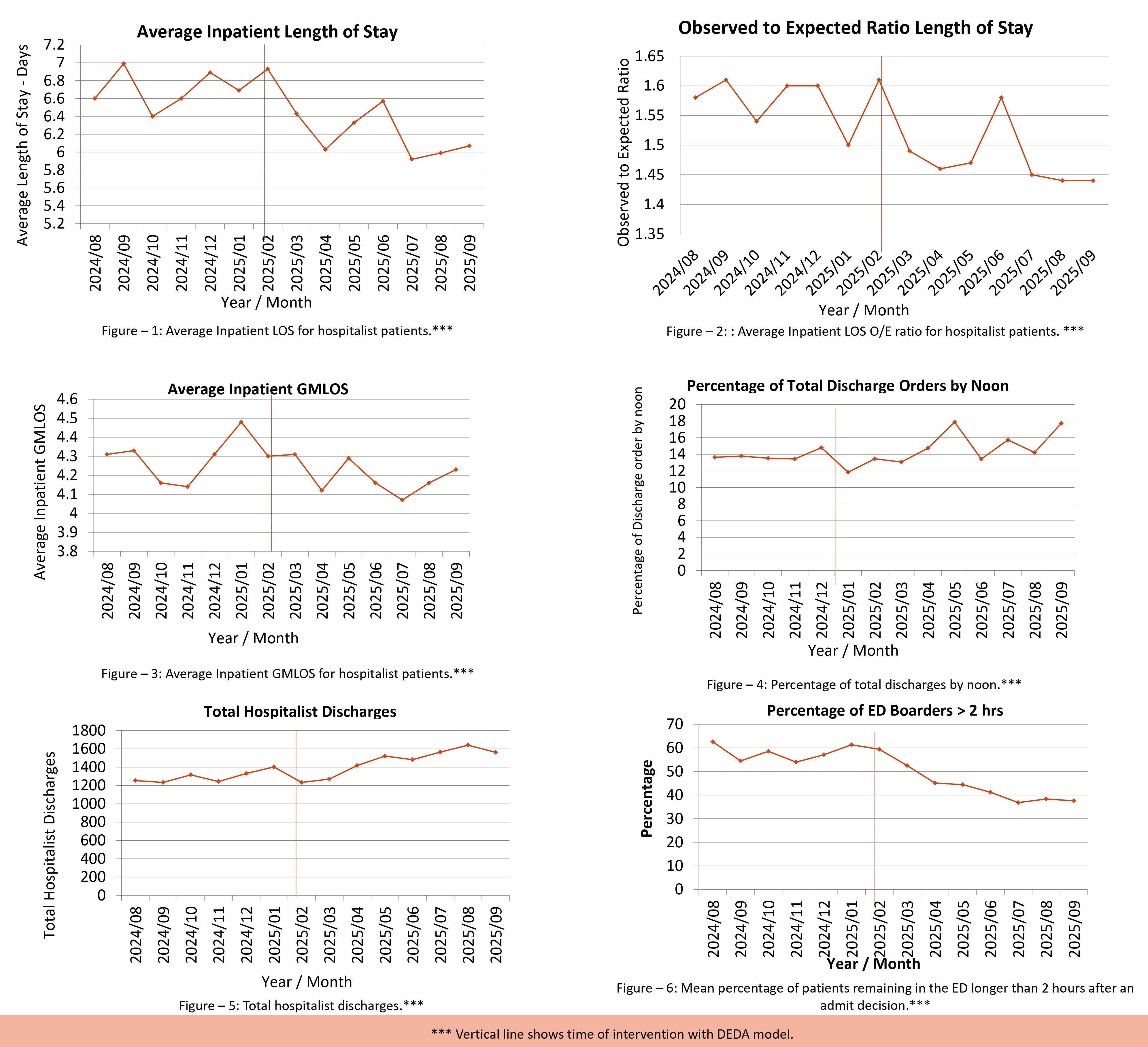
Description: After the implementation of the DEDA model, we noted statistically significant improvements in hospitalist metrics. LOS decreased by 0.5 days from 6.7 to 6.2 days (95% CI 0.26–0.81, p< 0.05), LOS O/E ratio improved by 0.10 from 1.57 to 1.47 (95% CI 0.04–0.15, p< 0.05), GMLOS improved by 0.1 from 4.29 days to 4.19 days (95% CI –0.20–0.22, p=0.09), mean percentage of discharges by noon increased by 1.7% from 13.5% to 15.2% (95% CI 0.0004–3.5, p=0.05), and mean monthly discharges increased by 206 discharges per month from 1,287 discharges per month to 1,493 discharges per month (95% CI 93–319, p< 0.05) (Figures: 1 - 5). ED metrics showed statistically significant improvements with a 15.9% decrease (95% CI 10.60–21.23, p< 0.05) in the percentage of patients staying in the ED >2 hours post-admit decision (Figure – 6), 11.2% decrease (95% CI 7.32–15.13, p< 0.05) in the proportion of admitted patients with ED stay >280 minutes (from 65.67% to 54.44%), 92.4 minute reduction (95% CI 57.81–127.04, p< 0.05) in time from admission decision to ED departure (202.5 minutes to 110.1 minutes) and 58.5 minute reduction (95% CI 25.32–91.81, p< 0.05) in total ED LOS for admitted patients (365.0 minutes to 306.4 minutes).
Conclusions: Our results show that the DEDA model led to significant improvements in hospitalist performance metrics, such as improved inpatient LOS, discharge efficiency, and patient throughput. As dedicated admitting hospitalists focused on ED admissions, rounding hospitalists could focus on inpatient care and discharges. It also improved ED efficiency and helped reduce ED Boarding times, and improved ED throughput. We found that a dedicated admission team in a high-volume tertiary care setting and peak ED hours can help optimize patient flow and resource utilization. The DEDA model may serve as an efficient and cost-effective intervention for hospitals experiencing ED congestion, boarding delays, and increased LOS.