Background: Severe hypertriglyceridemia (triglyceride >1000 mg/dl) occurs at a rate of 0.4% and is associated with a range of medical complications including severe pancreatitis and its complications like acute kidney injury . Hypertriglyceridemia (HTG) is the third most common cause of acute pancreatitis especially in levels above 1000 mg/dl. It has been suggested that insulin and plasmapheresis have a role in the management of acute HTGP, but there are no clear guidelines on the best treatment option in terms of better clinical outcomes. We present a retrospective study of patients who received active treatment in the form of insulin drip, plasmapharesis or a combination of both versus supportive treatment alone
Methods: We reviewed medical records on patient’s age > 18 years, admitted with the primary diagnosis pancreatitis and had TG level above 1000 mg/dl between Jan 2014 and Oct 2017. We gathered information on demographics, co-morbidities, incidence of pancreatitis associated with alcohol and type of treatment received. Outcomes were hospital length of stay (LOS) and recurrence of HTG induced pancreatitis (HTGIP).
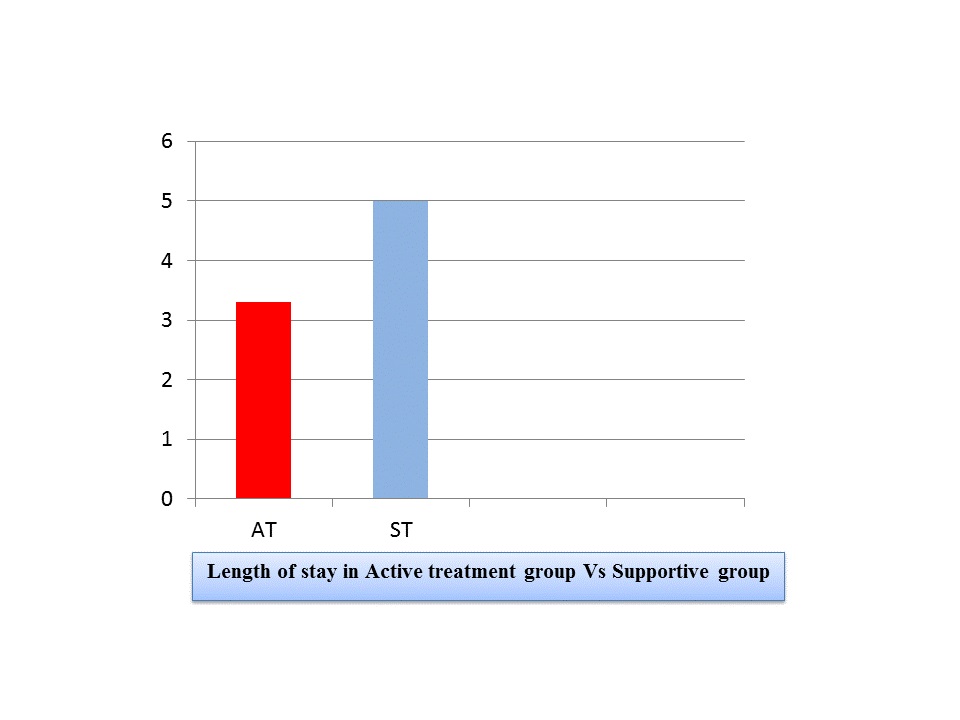
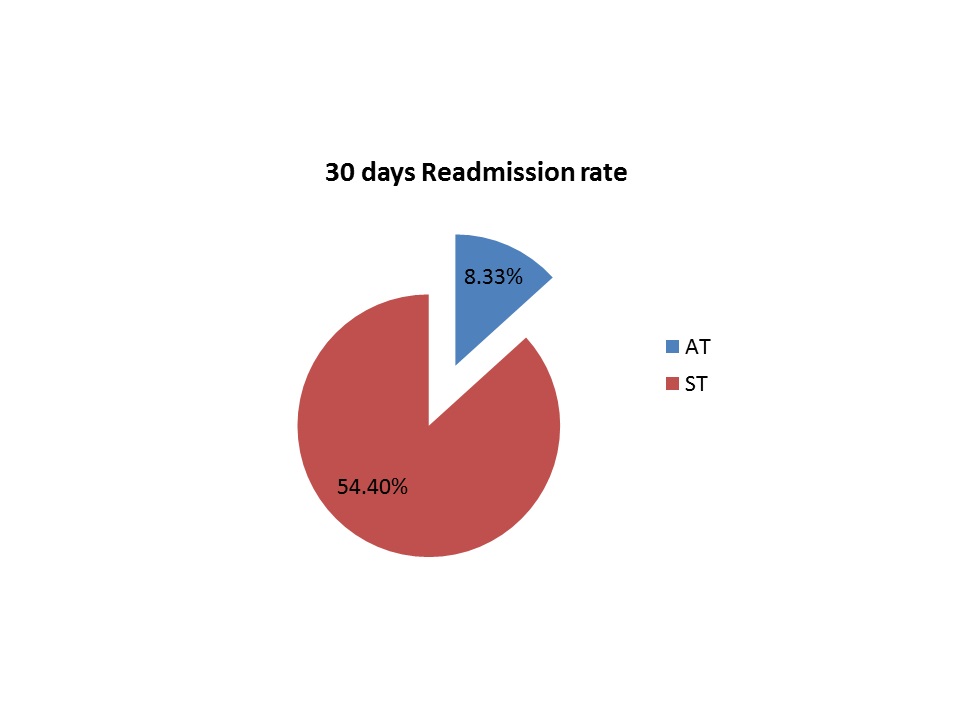
Results: 89 Patients had a HTG level of 1000 mg/dl and above, and from that 36 had a diagnosis of acute pancreatitis. The Incidence of HTGIP among Patients with ETOH abuse is 41%. The mean age of presentation was 44.8; there was a predominance of men (88%) and Hispanic population (44.8%). 54.3% (19) were treated with supportive treatment (ST) and had a mean TG of 1614.79 mg/dl versus 45.7% (16) were given active treatment (AT) with a mean TG of 3066.19 mg/dl. Total LOS was less in AT group with a mean of 3.3 days versus 5.0 days in ST group (p=0.001). The days needed to achieve TG level below 500 was significantly less in the AT group (4.56 versus 1.56 in ST group) (p= 0.010). The 30 day readmission rate in ST group was 54.4% versus 8.33% in AT group ( P= 0.016).
Conclusions: Hospital LOS in patients receiving active treatment was shorter than supportive treatment. They also have a lower readmission rate and faster achievement of TG lower than 500 mg/dl, suggesting more effective therapy in the AT group. We also observed high percentage of comorbid alcohol use with TG level above 1000 mg/dl.
We suggest starting active treatment in any patient with HTG- induced pancreatitis if TG level is equal or above 1000mg/dl, which may favor insulin drip in diabetes patients and plasmapheresis in non-diabetics. Further, we propose checking TG level in any diagnosis of acute pancreatitis even if alcohol abuse is present as HTG is frequently found.