
Background:
There has been little work on the impact of hospitalist involvement in short‐stay or observation units. In August 2005, the University Hospital consolidated the care of medical observation patients onto a hospitalist‐run, nonteaching “clinical decision unit“ (CDU), a separate 10‐bed, 23‐hour observation unit. The rationale was that the care of patients in a dedicated unit would be more efficient than the care on an inpatient medicine service. The chest pain unit, formerly staffed by cardiology, also became part of this unit. The purpose of this study was to examine the impact of this unit on length of stay.
Methods:
The 5 most common CDU diagnoses were identified based on discharge data and included chest pain, asthma, syncope, cellulitis, and pyelonephritis. Patient acuity was assessed by use of 3M APR‐DRG methodology. We identified patients discharged with these 5 diagnoses in the 12 months prior to the unit creation and compared their length of stay (LOS) with patients admitted with the same diagnoses for 12 months after implementation. About one third of these patients were admitted to the CDU, with the rest to the inpatient medicine service. We also compared the LOS for patients with each diagnosis admitted to the CDU versus those admitted to the inpa‐tient service for the 12 months after implementation.
Results:
The overall LOS for all patients with these diagnoses (regardless of admission location) decreased from 2.4 to 2.2 days (P = .05) between the 12‐month pre‐and postimplementation periods. The greatest decreases were seen for patients with cellulitis (from 2.4 to 1.9 days, P < .001) and asthma (from 2.2 to 1.2 days, P < .001). The differences in overall LOS for patients with chest pain, pyelonephritis, and syncope were not significant. During the 12 months after implementation, there were significant differences between the LOS for patients with each of these diagnoses admitted to the CDU versus those admitted to the inpatient medicine service (Table 1). The acuity of patients admitted to the medicine service was greater for all diagnoses except asthma.
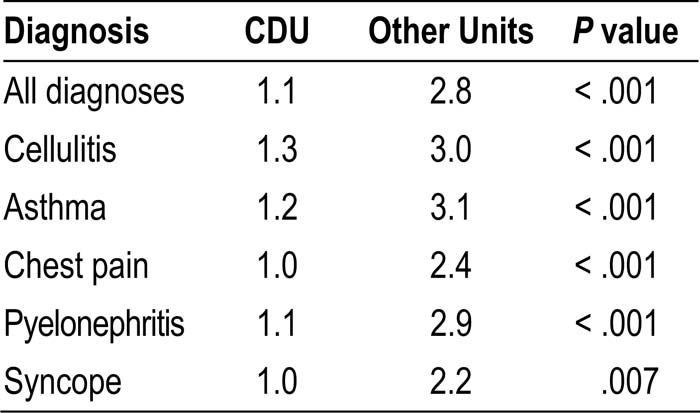
Table 1. LOS for CDU Versus Inpatient Unit
Conclusions:
Implementation of a hospitalist‐run observation unit was associated with a significantly decreased LOS for patients presenting with chest pain, cellulitis, asthma, pyelonephritis, and syncope. The decreased acuity of patients admitted to the CDU demonstrates appropriate unit utilization.
Author Disclosure:
L. Leykum, none; S. Piwinski, none; T. Arevalo, none; W. Pao, none; V. Huerta, none; N. Ray, none.