Background: Hyperbilirubinemia is the most common cause of hospitalization among neonates. Severe, untreated hyperbilirubinemia can lead to acute bilirubin encephalopathy and kernicterus. Although rare, these conditions can pose significant risks for morbidity and mortality in neonates.In 2004, the American Academy of Pediatrics (AAP) issued a guideline for management of hyperbilirubinemia in neonates over 35 weeks gestation which emphasized the importance of systematic assessment of hyperbilirubinemia in neonates and timely intervention when appropriate.
Based on these guidelines, a new pathway for treating hyperbilirubinemia was launched for the inpatient pediatric unit at the Lehigh Valley Health Network on January 1st, 2018. The aim of the pathway was to institute a standardized approach to identifying and managing hyperbilirubinemia in neonates over 35 weeks of gestation to not only reduce the incidence of severe hyperbilirubinemia and its associated clinical morbidities, but also reduce the provider variability in practice and optimize the delivery of phototherapy while decreasing costs pertaining to length of stay and use of hospital resources.
Methods: A retrospective chart review was completed prior to implementation of the pathway and included about 70 neonates admitted for hyperbilirubinemia. The new pathway was implemented in January 2018, and data collection was continuously collected from the electronic medical record about the admission of the patient and their management on the pediatrics floor.
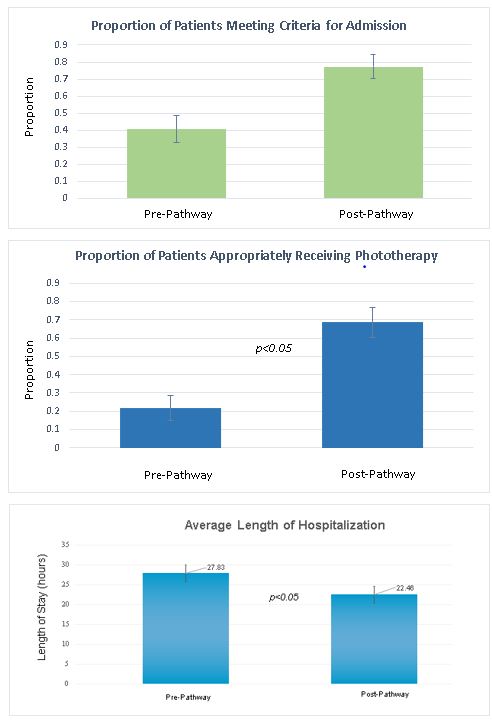
Results: Data collected after implementation of the pathway show improved risk stratification of admitted children, improvement in appropriate initiation of phototherapy, and shortened length of stay among patients hospitalized for hyperbilirubinemia, as demonstrated by the graphs below.
Conclusions: Based on these results, we conclude that the newly implemented hyperbilirubinemia pathway has effectively reduced unnecessary hospital admissions for hyperbilirubinemia, improved rates of appropriate initiation of phototherapy, and reduced length of stay. This indicates an improvement in risk stratification of patients and improvement in management of patients once admitted which has direct effects on patient safety. Furthermore, reductions in inappropriate treatment initiations suggest that that the pathway also may decrease unnecessary admissions, decreasing the exposure to possible hospital acquired infections and parental stress in the vulnerable neonatal population.