Background: Discharge of hospitalized patients is a multistep process, involving communication amongst numerous healthcare providers. Delays in discharge cause a backlog of patients in the ED and ICUs, leading to prolonged patient wait times and overcrowding in the ED. Furthermore, many discharges occur in the evening hours, when there is a covering provider. Our institution has no standardized protocol on relaying discharge information from residents to nurses and patients, other than a simple EMR-generated discharge medication list. In this project, our goal was to determine the baseline perception of the discharge process and implement a mandatory, standardized discharge instruction checklist accessible to nurses, residents, and patients.
Methods: Baseline surveys to determine problems with the discharge process were sent via email to nurses on general medicine floors and to all Internal Medicine residents. A discharge checklist was developed based on the issues identified. The checklist was launched during a resident safety conference, and we worked with our EMR representatives to make sure the list was included in patients’ discharge paperwork, which is visible to all physicians, nurses, and patients. Residents were required to complete this checklist prior to printing the AVS.
Results: The survey was completed by 86 nursing staff and 48 residents. For both residents and nurses, >95% have encountered discharge related issues. For nurses, 84.9% found inconsistencies in discharge related documentation, 89.5% have been contacted by patients after discharge and the most common issues were: discharge medication, transportation, and follow-up. Among residents, 91.7% had been contacted by nurses during cross cover to clarify discharge plans, 95.8% were willing to complete a discharge checklist and the most common issues were: medication refills, opioid prescriptions and follow-up. Both nurses (94.2%) and residents (81.3%) agreed that a standardized discharge template would be beneficial.
Conclusions: The majority of nurses and residents perceive a lack of standardized discharge communication. This ineffective communication can have a significant impact on a patient’s health. The discharge related issues seen in the survey, specifically medication related questions, were similar to what have been reported in literature. Prior studies have also identified ineffective communication as the underlying reason for adverse events after discharge.
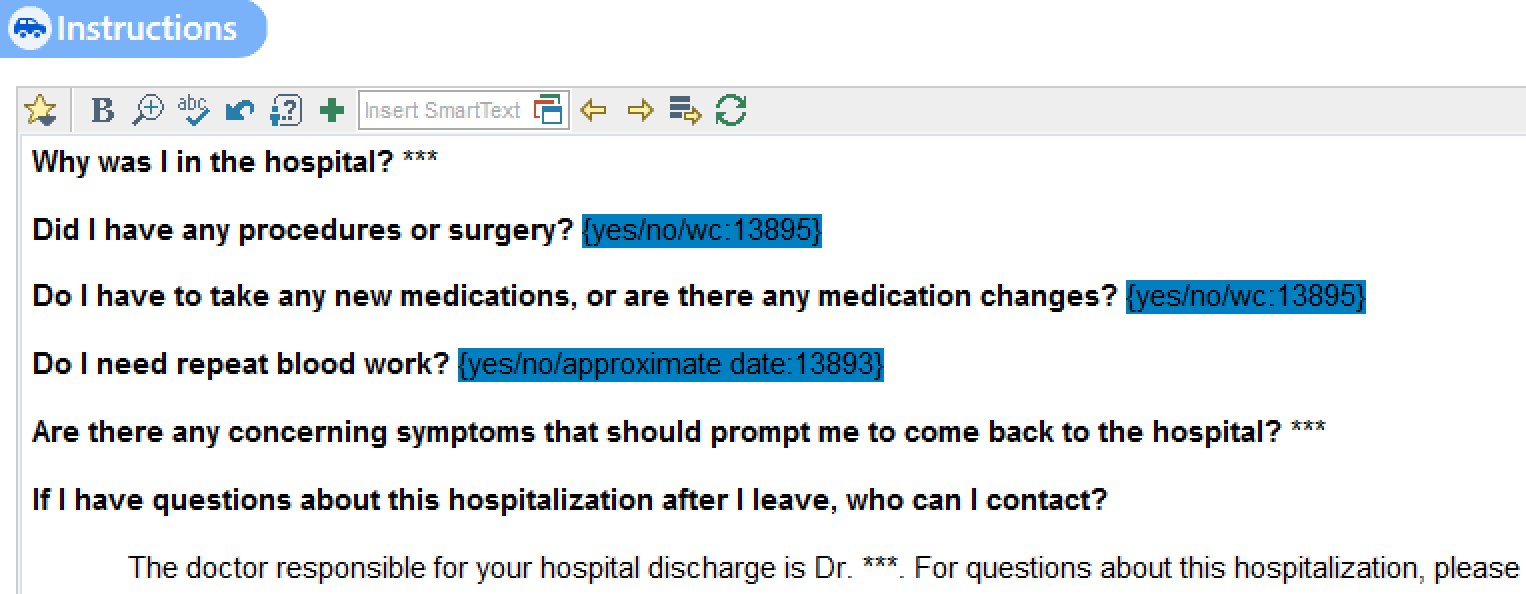
The openness of nursing and residents in the implementation of a standardized checklist is key for improvement. Our checklist includes the reason for admission, medication changes, follow-up and contact person after discharge, all written in patient-friendly language. We hope that our checklist will provide clearer discharge plans for both patients and providers, and ultimately help prevent adverse events. To determine its efficacy, a post-intervention survey is being developed for residents and nurses.