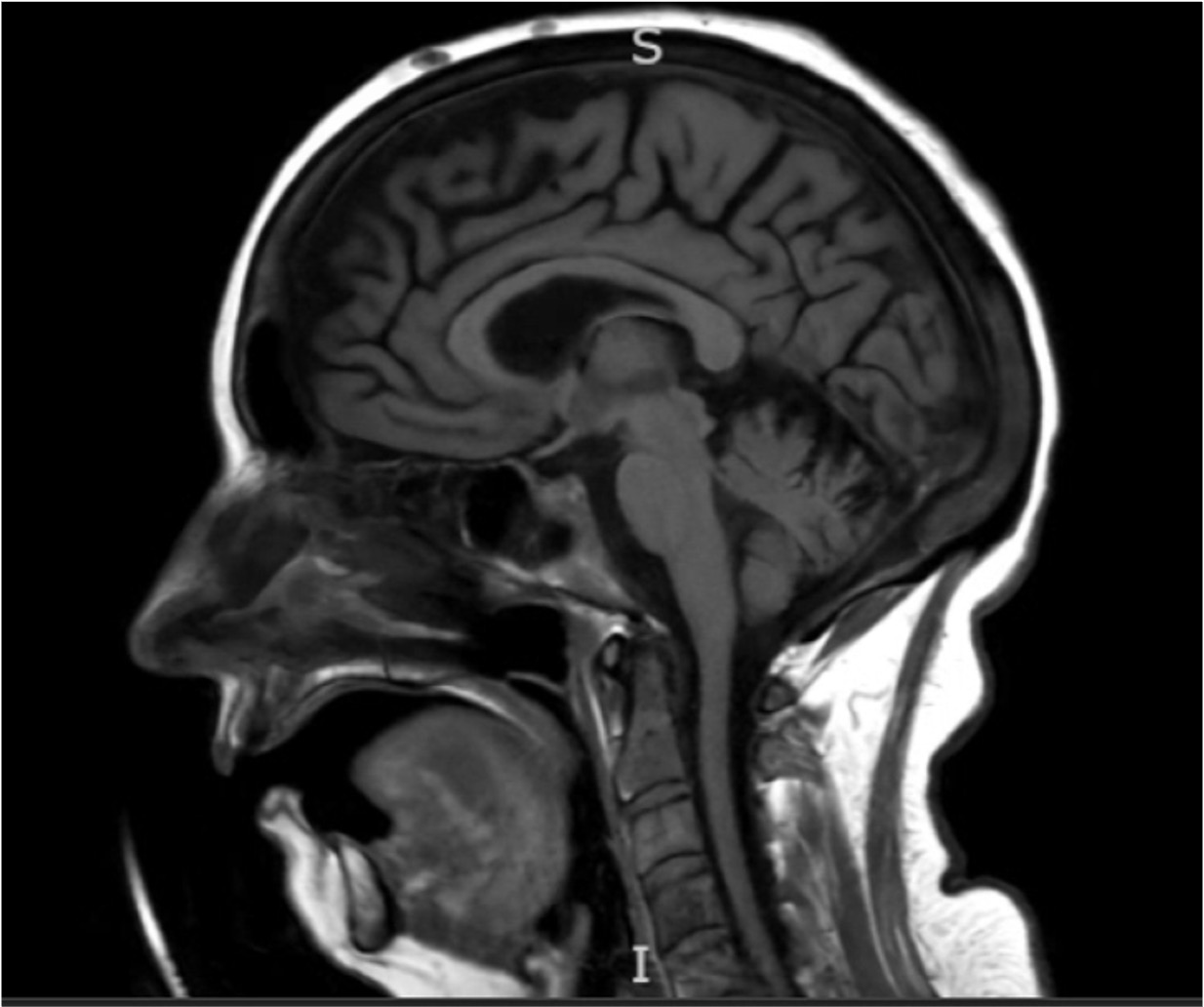
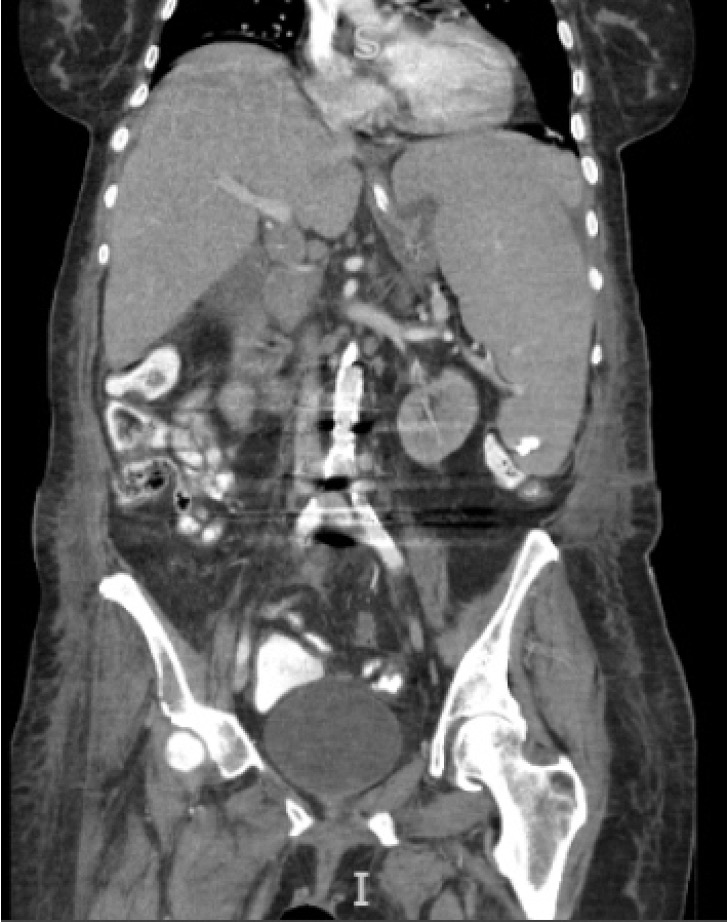
Case Presentation: A 75-year-old independent female presented with abdominal pain, confusion, lower back pain, and difficulty walking. Upon admission, temperature was 100.9ºF, heart rate was 85 bpm, blood pressure was 184/72, and respiratory rate 16 with oxygen saturation of 96%. Physical exam was remarkable for fluctuating mental status. Laboratory evaluation was significant for a lactic acid of 4.1 mmol/L, calcium of 14.8 mg/dL, albumin of 3.2 g/dL, Vit D 25 of 11.1 ng/mL, PTH of 3.3 mg/mL. CT abdomen pelvis showed splenomegaly and multiple lytic bone lesions. Brain MRI revealed multiple calvarial enhancing lesions. Blood smear showed rouleaux formation, acanthocytes, and burr cells. The IgM level was 1327, and serum electrophoresis showed elevated IgM and B2 microglobulin. Bisphosphonates, IV fluids, and calcitonin were started, improving mental status. She was also pancytopenic, requiring multiple RBC and platelet transfusions. She developed spontaneous tumor lysis syndrome with AKI while awaiting bone marrow biopsy which confirmed lymphoplasmacytic lymphoma/Waldenström’s macroglobulinemia. Multiple family meetings were held to clarify and update the goals of care. She was previously functional, and her goals included returning to independent living, avoiding long-term dialysis, intubation or resuscitation. Chemotherapy response was a reasonable possibility and rituximab and cyclophosphamide were started inpatient. Since she developed anuric AKI requiring HD, prior goals were revisited, and she agreed to time-limited HD. Due to her clinical status, she required daily long dialysis sessions, which required conscious planning with the family to maximize visitation time. Given the persistent need for transfusions, she developed progressive volume overload which impacted her respiratory status. A partial response to high-dose diuretics showed promise for renal recovery. However, she deteriorated over the next week until the decision was made to transition to comfort care. She passed shortly afterwards. The family was grateful to the team for their continued support, respecting her goals of care and ultimately helping in the transition when recovery was no longer possible.
Discussion: Lymphoplasmacytic lymphoma is a rare subtype of Non-Hodgkin Lymphoma, with a median age at diagnosis of 70 years, and 95% of patients have IgM secretion and are categorized as having Waldenström macroglobulinemia (WM) (1). The typical presentation of WM involves weakness, fatigue, weight loss, bone pain, and splenomegaly (2). Laboratory findings include anemia, elevated monoclonal protein, serum β2 microglobulin, LDH, MYD88, or CXCR4 (3). Diagnosis is made by bone marrow biopsy (4). In early stages, surveillance alone is recommended; however, aggressive variants require symptomatic chemotherapy (5,6). When clinical status changes rapidly, navigating goals of care can be challenging. In such situations, constant open dialogue is vital. Physicians must balance practical compassion for the patient and emotional care for the family while respecting the patient’s original wishes alongside the family’s hope. For us, this looked like starting chemotherapy, revisiting dialysis wishes and ultimately explaining the need to transition to comfort care.
Conclusions: Lymphoplasmacytic Lymphoma is a rare, incurable malignancy that can progress rapidly. This case highlights that a constant focus on patient-centered care is the only way to navigate uncertainty effectively in the face of serious illness.