
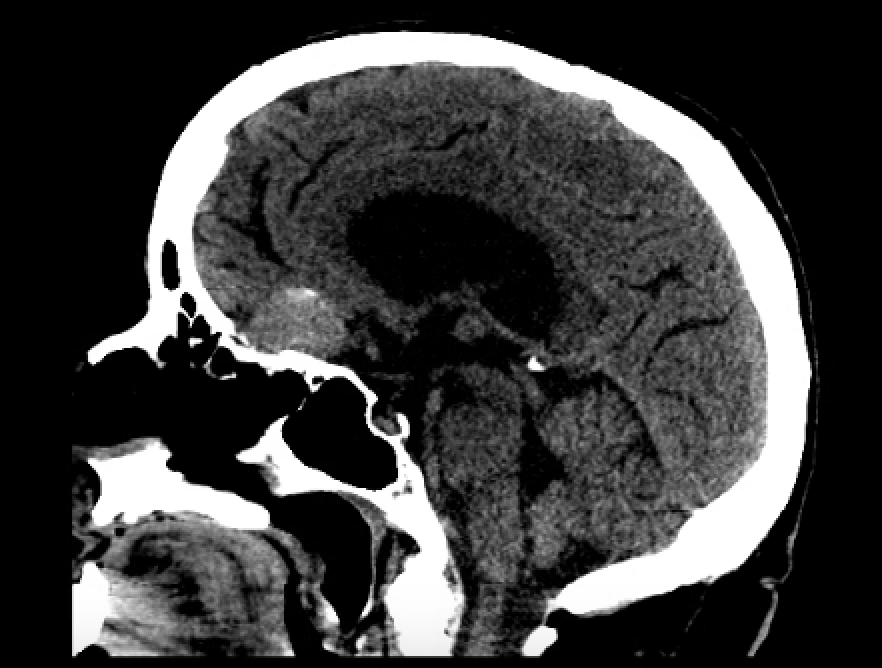
Case Presentation: A 71-year-old female presented to an outside hospital with altered mental status and fever. She was febrile (102 °F), tachycardic, and laboratory evaluation demonstrated leukocytosis. Blood cultures were drawn, and ceftriaxone and vancomycin were initiated empirically. CT of the head showed an olfactory groove meningioma. The patient was transferred to our institution for neurosurgical evaluation, given the suspicion that the mass was leading to altered mental status. Upon arrival, the patient was afebrile. Physical examination revealed persistent disorientation, but no focal neurological deficits. Laboratory studies revealed resolved leukocytosis and no other significant abnormalities. Repeat blood cultures at our facility demonstrated no growth. Original blood cultures grew Enterococcus avium. The patient reported routinely feeding birds in her backyard. The patient was initiated on intravenous ampicillin. Neurosurgery recommended outpatient follow-up for potential intervention on the suspected meningioma.
Discussion: Enterococci are a diverse group of bacteria found in humans, animals, and the environment. E. avium accounts for only 1% of all enterococcal infections in humans (1-2). It commonly presents as bacteremia with other manifestations, including endocarditis, urinary tract infections, osteomyelitis, and rare CNS infections (3). The presenting findings include fever, altered mental status, or sepsis. E. avium is generally susceptible to ampicillin and vancomycin. For severe infections, prolonged intravenous antibiotic therapy is recommended (3-4). Crude mortality is approximately 24%, and infection-attributable mortality is approximately 11% in the bacteremia series (1, 4). Meningiomas are slow-growing, benign, extra-axial tumors, and characteristic MRI findings are sufficient for diagnosis (5). Symptoms include headache, progressive focal neurological deficits, seizures, visual disturbances, and cognitive or personality changes (6). Meningiomas do not cause fever, and acute altered mental status is an infrequent presentation, mainly attributable to hemorrhage or infarction, which was not appreciated on imaging.Medical errors are present in approximately 6-7% of all hospital admissions, and bias, or mistakes in systematic thinking, lead to at least half of them (7). Anchoring and confirmation bias are among the most common, and this case offers a great opportunity to illustrate these biases. Anchoring is the tendency to rely too heavily on the first piece of information encountered when making subsequent judgments. We could have focused on the reason for transfer, the CNS mass, and disregarded the initial confusion and fever. Confirmation bias is the tendency to seek, interpret, and remember information that confirms one’s preexisting beliefs (8). For example, we could use the repeat negative infectious workup as our cue to disregard the initial presentation of the patient. Only by a diagnostic time-out, revisiting all available information, and following up on the blood culture results at the transferring facility were we able to identify and appropriately treat E. avium.
Conclusions: Clinicians must remain vigilant to confirmation and anchoring biases. The meningioma could have been presumed to explain the patient’s symptoms, potentially delaying the proper management of E. avium. Understanding the typical presentations and the appropriate use of a diagnostic time-out are critical for accurate diagnosis and management.
.png)