Background: The use of imaging is highly prevalent in hospitalized patients with about two images performed on every hospitalized patient (Levin et al). While imaging is utilized for specific indications, incidental findings are common with 45.0% of chest CTs resulting in incidentalomas (O’Sullivan et al). Lack of appropriate follow up to incidental findings (IFs) leads to delays in diagnosis and treatment. Previous literature on incidental findings has focused on masses or “incidentalomas.” Incidental findings as a whole, including masses, anatomic abnormalities (AA), medical conditions (MC), and foreign bodies (FB), is an unstudied medical phenomenon. We sought to categorize and determine the prevalence of IFs as well as to characterize the provider’s assessment and plan for those findings.
Methods: We reviewed a random sample of 153 patients from the 3,782 patients discharged between January 1 and June 30, 2018 from the Hospital Medicine service at Parkland Memorial Hospital, a 869 bed, academic safety net hospital in Dallas, TX. All x-ray (XR), computed tomography (CT), ultrasound (US), including echocardiogram, magnetic resonance (MR), and nuclear medicine (NM) studies ordered in the emergency department and during hospitalization were included. We assessed studies for type, reason, main findings, and IFs. We defined IFs as any finding found in the radiologists’ “Impressions” not related to the reason for imaging exam or the patient’s principal diagnosis and categorized them into masses, AAs, MCs or FBs. Progress notes one day after the imaging result date and discharge summaries were assessed for documentation of the IF. Follow up was assessed post-discharge and for one year after discharge. Patient adherence to follow up plans was also captured. Any progression or complications from IFs were assessed.
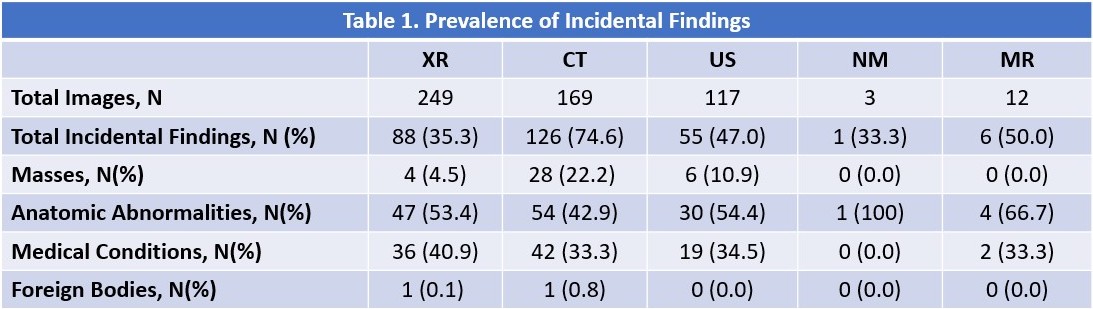
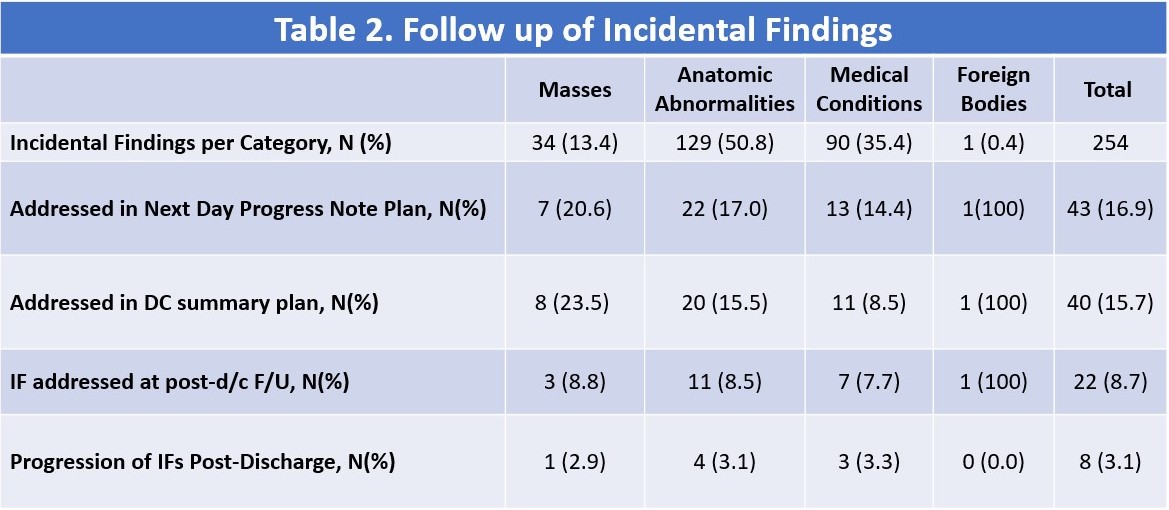
Results: We found a total of 246 IFs out of 550 total radiologic studies with an average of 1.6 IFs per patient. Each patient had an average of 3.6 imaging studies. XR was the most common (1.63/patient) with an IF prevalence of 35.0% while CT was the second most common (0.82/patient) with an IF prevalence of 74.5%. While only 2% of imaging was MR, it had an IF prevalence of 50.0%. Anatomic abnormalities were the most prevalent (42.8% of IFs on CT, 53.4% on XR, 54.5% on US), followed by medical conditions (33.3% on CT, 40.9% on XR, 34.5% on US) and masses (22.2% on CT, 4.5% on XR, 10.9% on US). One incidental foreign body was seen. (Table 1)20.6% of patients with masses had the IF noted on the next progress note and 23.5% had plans in the discharge summary (Table 2). Of the non-mass IFs, 16.4% of patients had the IF noted on the next day progress note and 14.5% had plans in the discharge summary. Nine of the patients showed progression of an IF on subsequent follow up, none of which were felt to be preventable. There were no deaths related to missed IFs.
Conclusions: Incidental radiographic findings are common in hospitalized patients. The majority of IFs were not specifically addressed in the discharge plan or in follow up. However, the clinical relevance of many of the IFs is unclear and the “signal to noise” ratio may be diminished. Risk stratifying IFs may help to increase the signal to noise ratio and call notice to IFs that are high risk and require close and reliable follow up.