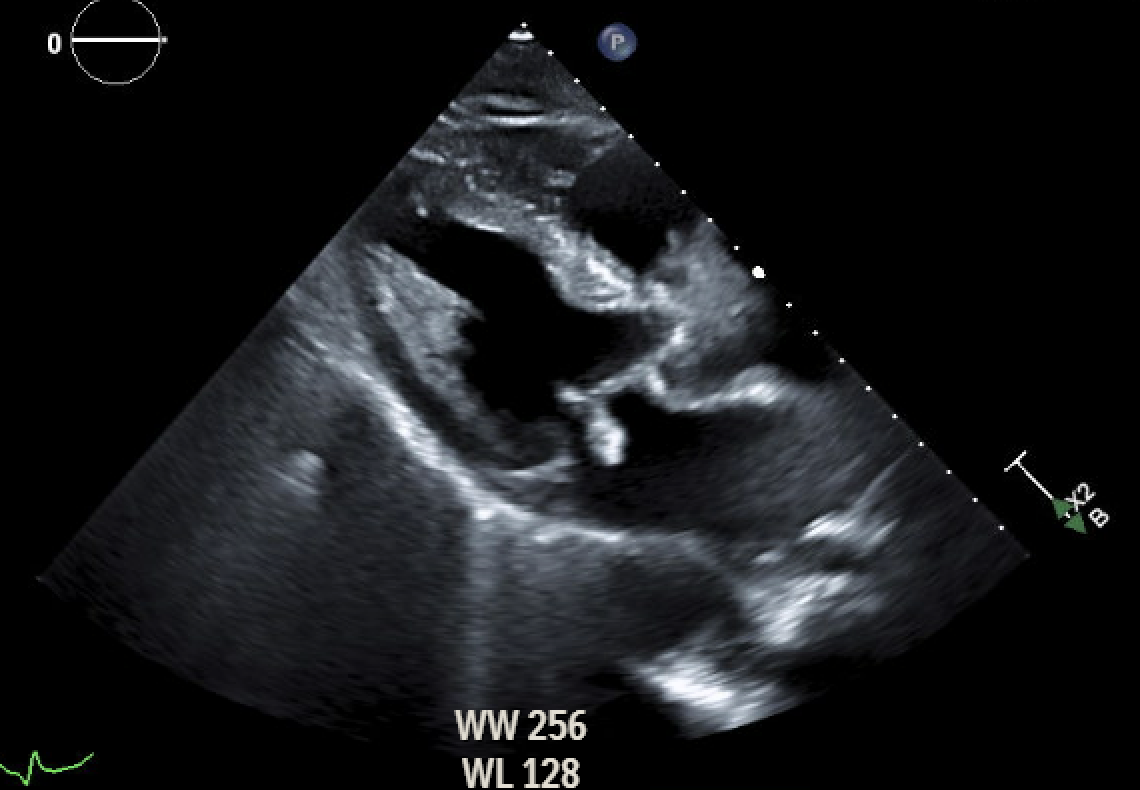
Case Presentation: A 65-year-old male with a history of hypertension, hyperlipidemia, gout, chronic rhinosinusitis, and lumbar spinal stenosis with a recent lumbar laminectomy presented with fatigue, hemoptysis, weight loss, and a new purpuric rash with hemorrhagic bullae. On initial blood work, he was found to be in acute renal failure, suspected of being intrinsic due to underlying vasculitis, given significant proteinuria and hematuria. There was also concern for possible IE given a new systolic murmur heard on examination. An echo was obtained, which showed a small vegetation versus mass on the aortic valve and another mass on the anterior mitral valve leaflet measuring approximately 3.2 cm x 1.6 cm. A punch biopsy of the lower extremity rash was performed, which was consistent with leukocytoclastic vasculitis, and the autoimmune panel was positive for cANCA and Proteinase-3 Ab. Treatment options at this time became a question of debate as blood cultures remained negative and no clear source of infection was determined. The patient was transferred to a tertiary care facility and underwent an aortic and mitral valve replacement. Valve tissue cultures grew Streptococcus gallolyticus, confirming the diagnosis of IE. He was treated with a long course of IV antibiotics and referred for colonoscopy due to concern for underlying malignancy.
Discussion: The high prevalence of Antineutrophil cytoplasmic antibody (ANCA) positivity in IE is clinically significant as it can lead to diagnostic confusion. ANCA positivity is found in approximately 18-43% of patients with IE. Culture-negative endocarditis with positive ANCA is even more of a diagnostic challenge. Misdiagnosis can lead to improper treatment. The importance lies in the difference in management. Endocarditis is managed with antibiotics, and vasculitis is managed with steroids. Delaying one management step can worsen the patient’s outcome. So differentiating between the two promptly is critical.
Conclusions: This case highlights the complexity of distinguishing ANCA-associated vasculitis from IE in patients with systemic symptoms, rash, renal involvement, and cardiac lesions. Valve cultures remain critical for diagnosing culture-negative endocarditis. Multidisciplinary coordination enabled timely surgical intervention and recovery. Early multidisciplinary collaboration and timely surgical intervention enabled effective management and recovery. This case reinforces the need for clinicians to maintain a high index of suspicion for IE in ANCA-positive patients with multisystem involvement, particularly when blood cultures are negative.