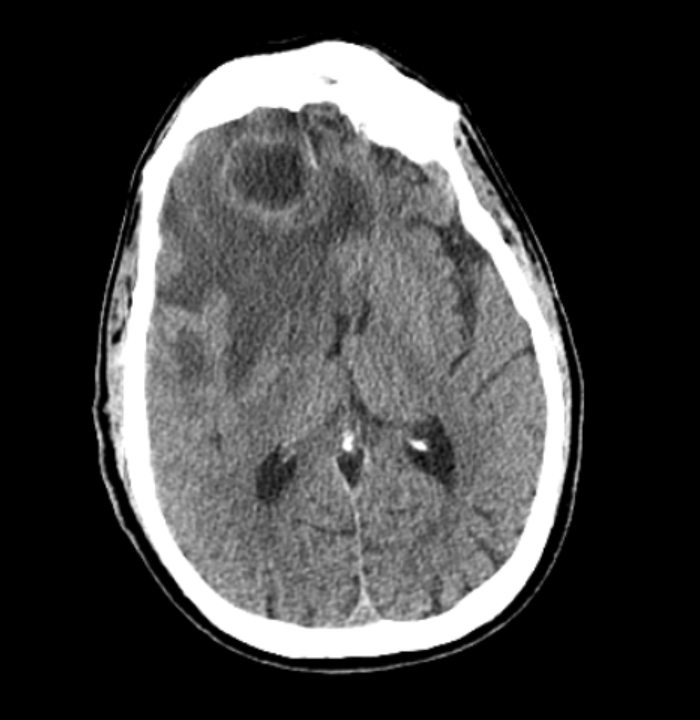
Case Presentation: A 65 year old male with myelodysplastic syndrome (SF3B1 mutation) on darbepoetin and luspatercept and a history of brain abscess secondary to dental infection with prior bilateral ethmoidectomies and maxillary antrectomies presented after a welfare check revealed altered living conditions and new slurred speech. On arrival, he was afebrile, bradycardic, and hemodynamically stable. Neurological exam showed facial asymmetry and lower extremity weakness. CT head demonstrated a right frontal lobe fluid containing lesion with vasogenic edema and 11 mm midline shift. MRI confirmed a large right frontal lobe abscess with extensive edema and 2.2 cm midline shift. He underwent right frontal craniotomy with neuronavigation for abscess resection. Subsequent CT facial bones revealed severe frontal bone osteomyelitis with posterior wall erosions of the left frontal sinus, intracranial communication, and bilateral medial orbital wall erosions.
Discussion: This patient presented with recurrent intracranial infection, ultimately diagnosed as a large right frontal lobe abscess. His history of prior brain abscess from dental infection, chronic sinus disease, and prior craniofacial surgeries created a predisposition for recurrence.Frontal bone osteomyelitis is a rare but recognized complication of sinusitis, often described in association with Pott’s puffy tumor—a subperiosteal abscess with underlying osteomyelitis. Although uncommon in the antibiotic era, several reports highlight its potential to progress to intracranial complications including epidural empyema, subdural empyema, and brain abscess. Tuon et al. described a case of frontal osteomyelitis complicated by brain abscess due to Staphylococcus aureus, underscoring the severity of direct extension from sinus disease. Similarly, recent case series emphasize that frontal sinusitis can lead to devastating outcomes when osteomyelitis erodes bony barriers, allowing spread into intracranial and orbital spaces.In our patient, the absence of fever or leukocytosis despite a large abscess reflects the blunted inflammatory response seen in immunocompromised hosts, such as those with myelodysplastic syndrome. The degree of vasogenic edema and midline shift placed him athigh risk for rapid neurological deterioration, necessitating urgent neurosurgical intervention. The persistence of osteomyelitis with bony erosions explains the recurrence of abscess formation and highlights the importance of considering chronic sinus disease and prior surgical changes as ongoing risk factors.This case aligns with published literature in demonstrating that frontal bone osteomyelitis can serve as a direct conduit for intracranial infection, leading to recurrent brain abscesses. Recognition of this pathway is critical, as delayed diagnosis can result in persistent infection, neurological deficits, and high morbidity. Early neuroimaging, surgical intervention, and multidisciplinary management are essential to prevent recurrence and optimize outcomes
Conclusions: Frontal bone osteomyelitis with direct intracranial spread is a rare but serious cause of recurrent brain abscess. This case emphasizes the importance of timely neuroimaging, surgical intervention, and vigilance for osteomyelitis in patients with prior sinus disease or craniofacial surgery. Early recognition of bony erosions and communication pathways is essential to prevent recurrence and optimize outcomes in immunocompromised patients.