Background: Prolonged hospital length of stay (LOS) and extended observation time negatively affect patient flow, resource utilization, and emergency department (ED) efficiency. Observation patients held in the ED often face delays in diagnostic testing, inconsistent care processes, and limited bed availability, contributing to system-wide congestion and increased healthcare costs. To address persistent ED overcrowding and high LOS, the hospital developed a Clinical Decision Unit (CDU) designed to streamline evaluation, provide protocol-driven care, and expedite final disposition.
Purpose: The aim of this innovation was to implement and refine a dedicated CDU to reduce observation LOS, decrease unnecessary inpatient admissions, improve ED throughput, and enhance coordinated, multidisciplinary care.
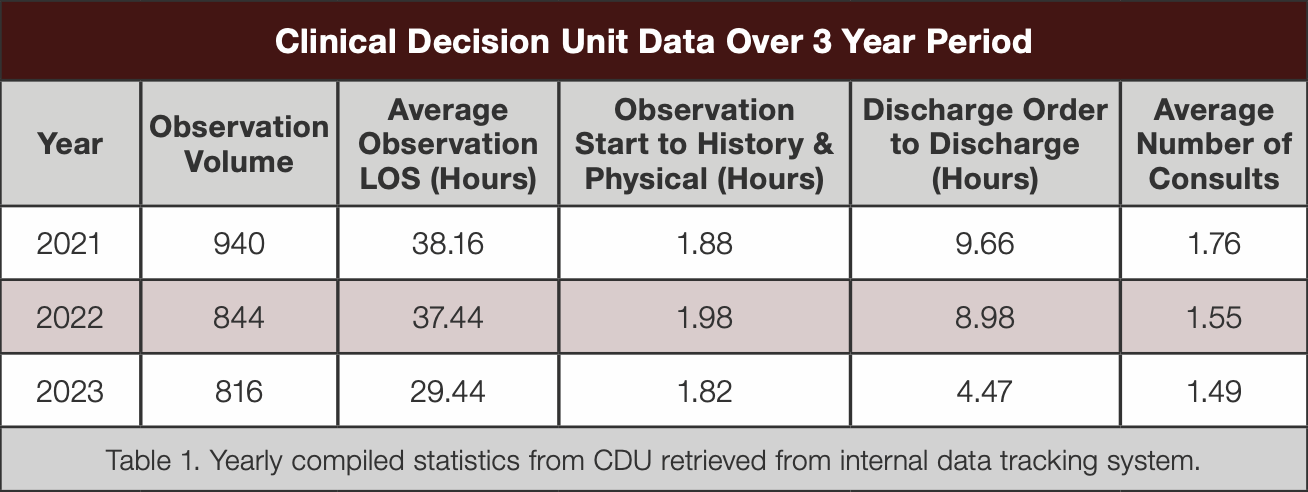
Description: A CDU was established on a medical–surgical unit with dedicated nursing staff, standardized workflows, and close collaboration among the ED, hospitalists, care management, and consulting services. Mission control tools (e.g., InterQual, Milliman) were used to determine observation status within minutes of ED presentation. A physician advisor reviewed cases when conversion to inpatient status was warranted.The CDU operated with a flexible staffing ratio of 5–10 patients per nurse or physician, depending on volume. Common CDU presentations included chest pain, abdominal pain, syncope, atrial fibrillation, transient ischemic attack, and heart failure exacerbations. Standardized protocols guided imaging, labs, consults, and reevaluation intervals. LOS, CDU volume, and consult utilization were continuously tracked through an internal system. Over time, workflow refinements were introduced, including multidisciplinary rounds, reduced extraneous testing, and structured physician-to-physician consults.
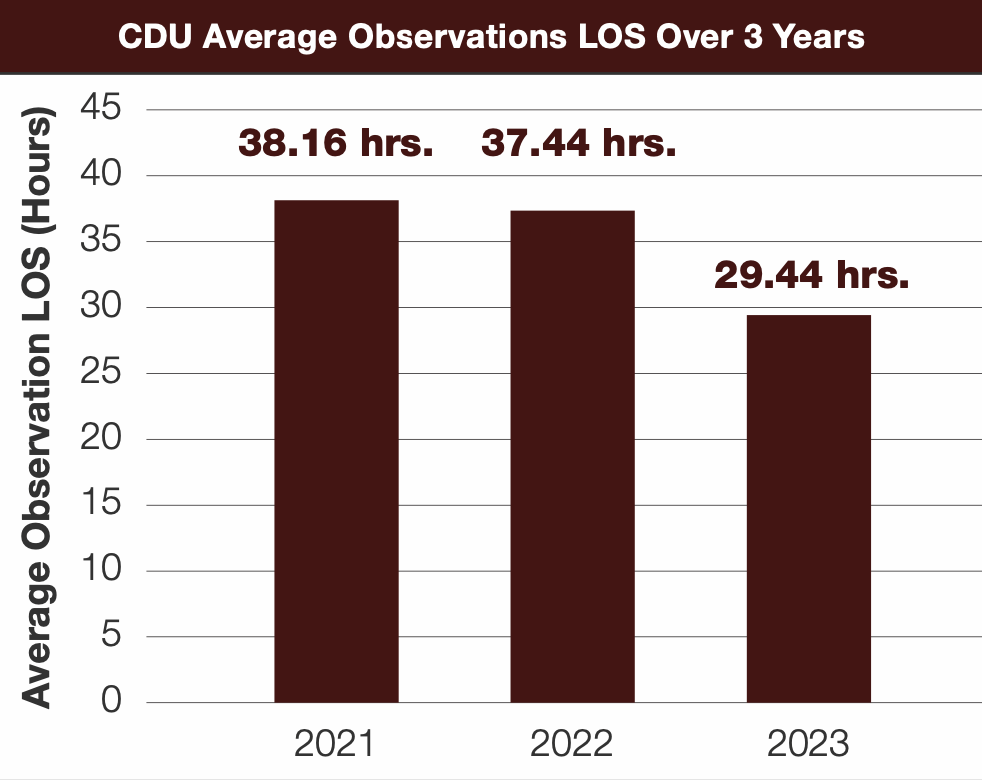
Conclusions: Implementation of a CDU led to a sustained reduction in observation LOS over a three-year period. Average LOS decreased from approximately 38 hours in 2021 to under 29 hours in 2023, reflecting a nearly 28% overall reduction. Consult utilization similarly decreased, and patient volume remained stable, demonstrating that LOS improvements were achieved without reducing patient throughput. The structured, protocol-driven model improved coordination, reduced ED crowding, and supported more efficient clinical decision-making. Continued emphasis on standardized workflows, targeted resource use, and multidisciplinary communication may further optimize LOS and CDU performance. This innovation highlights the value of dedicated observation units as effective operational strategies for improving hospital throughput and patient care efficiency.