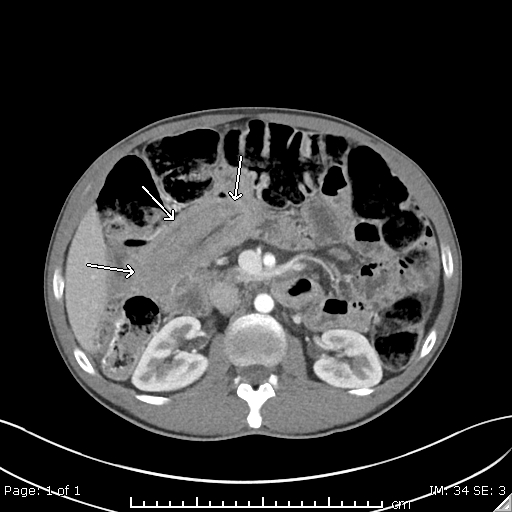
Case Presentation: A 42-year-old man presented to his primary care clinic with five weeks of diarrhea with up to 8 loose, watery stools a day and cramping abdominal pain. On exam patient was well appearing, with normal vital signs, no abdominal tenderness or distention. Laboratory evaluation revealed a hemoglobin of 12.4 g/dL, albumin of 3.3 g/dL, C-reactive protein of 1.07 mmol/L and otherwise unremarkable complete blood count and complete metabolic panel. A computed tomography (CT) scan demonstrated a 10cm segment of intussusception in the jejunum, other small intussusceptions and dilated fluid filled loops of jejunum. He was referred to the Emergency Room and evaluated by General Surgery. He had a benign abdominal exam and no signs of obstruction and discharged home with a referral to Gastroenterology. Further laboratory testing repeats a ferritin of 3 ng/mL and a tissue transglutaminase antibody of > 100 U/mL. Push enteroscopy showed scalloped mucosa in the duodenum and jejunum and biopsies with increase intra-epithelial lymphocytes and blunted villi. Ileocolonoscopy was endoscopically normal with biopsies showed increased lymphocytes in the ileum and colon. The biopsies confirmed extensive celiac disease (CD) and lymphagenous colitis, a type of microscopic colitis. He was counseled on maintaining a gluten free diet with improvement of his initial symptoms. Repeat CT scan showed resolution of his intussusception and he reported an improvement in loose stools.
Discussion: CD is a chronic immune-mediated response to gluten resulting in small bowel injury, nutrient malabsorption, and often gastrointestinal symptoms. It has an estimated prevalence of 1% of the population worldwide. People with CD can be asymptomatic or have presenting signs and symptoms that are widely variable and can be vague. Intussusception is when a part of the intestine telescopes into another segment of intestine and can range from asymptomatic to causing a bowel obstruction and a medical emergency. An intussusception can be caused by several benign and malignant conditions such as Crohn’s disease, infection, malignancy, or adhesions and often required endoscopic evaluation to confirm diagnosis. Intussusception is a very rare presenting symptom and complication of CD.
Conclusions: CD is a common auto-immune condition that can often evade diagnosis due to subtle or vague symptoms. Intussusception is a rare condition and even more rare to be the presenting presentation of celiac disease, occurring in less than 1% of all people with CD. This case illustrates the importance of keeping the differential broad and include celiac disease in the cases of patients presenting with small bowel intussusception. Early identification of CD in intussusception may allow for management with a gluten free diet and may avoid unnecessary surgery.