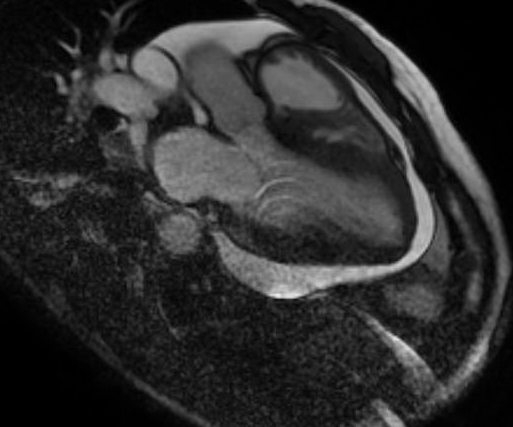
Case Presentation: A 43 year old male with a past medical history of stage 4 chronic kidney disease, hypertension treated with Minoxidil, former smoker, was initially diagnosed 9 years prior with presumed viral small pericardial effusion that remained stable on follow-up with serial echocardiograms. He presented with dyspnea and chest tightness with exertion, orthopnea, paroxysmal nocturnal dyspnea, peripheral edema, orthostatic lightheadedness of a few months duration. Pulmonary function studies showed moderate to severe airflow obstruction. Physical exam noted for jugular venous distention with positive Kussmaul’s sign suggesting significant pericardial effusion, but no pulsus paradoxus. There was no evidence of uremia. Immunologic studies were negative. A cardiac echo showed a moderate to large circumferential pericardial effusion, enlarged right sided heart chambers. Diagnostic and therapeutic pericardiocentesis with removal of 1200cc pink, fluid was performed. Laboratory evaluation of the fluid was unremarkable and cultures were negative. Follow up echo showed reaccumulation of fluid. Cardiac MRI confirmed large circumferential pericardial effusion with no evidence of thickening of the pericardium. Minoxidil was discontinued due to concern of Minoxidil induced pericardial effusion. Pericardial window was not performed as within 2-3 days the patient reported resolution of his symptoms and a follow up echocardiogram showed significant improvement of the fluid.
Discussion: Pericardial effusion is reported in patients undergoing dialysis and in those with normal renal function. Patients with renal impairment are at higher risk of developing pericardial effusion. Known cardiovascular side effects associated with the use of Minoxidil include T-wave changes 60%, edema (7% – 10%), pericarditis, pericardial effusion (3%) that may progress to tamponade, angina pectoris, cardiac failure, reflex tachycardia. Pericardial effusion has been frequently reported in patients undergoing dialysis, with patients using Monoxidil having a higher incidence (81% on Minoxidil versus no Minoxidil 23% p<0.0005). Patients with significant pericardial effusion leading to hemodynamic instability and cardiac tamponade usually present with signs and symptoms related to impaired cardiac function like dyspnea, elevated jugular venous pressure, positive Kussmaul’s sign, heart failure. In the absence of cardiac tamponade, most patients with a pericardial effusion have no symptoms and pericardial effusions are often diagnosed incidentally by echocardiography. Most cases of pericardial effusion resolve spontaneously upon cessation of Minoxidil. Discontinuation of Minoxidil resulted in the resolution of symptoms and pericardial effusion which prevented more aggressive means of pericardial drainage like pericardial window. Pericardiocentesis is required in patients with hemodynamic compromise.
Conclusions: The incidence of pericardial effusion is low, being reported in up to 3% of patients taking Minoxidil. However Minoxidil induced pericardial effusion should be considered in patients treated with this drug as medication discontinuation is associated with cessation of symptoms and resolution of pericardial fluid. Therefore other more invasive methods of pericardial fluid drainage can be avoided.