Background: The Institute of Medicine estimates that there are 44,000-98,000 preventable deaths per year. However, there is a paucity of literature regarding preventable death rates, despite its importance as a quality measure.
Methods: All deaths in the general medicine service from 2010-2012 at an academic hospital underwent an independent retrospective chart review by a physician and registered nurse. Extracted variables included admission risk of mortality based on APR-DRG, cause of death, potential preventability, and reasons for potential preventability. In cases of disagreement, an additional physician reviewer assessed the case.
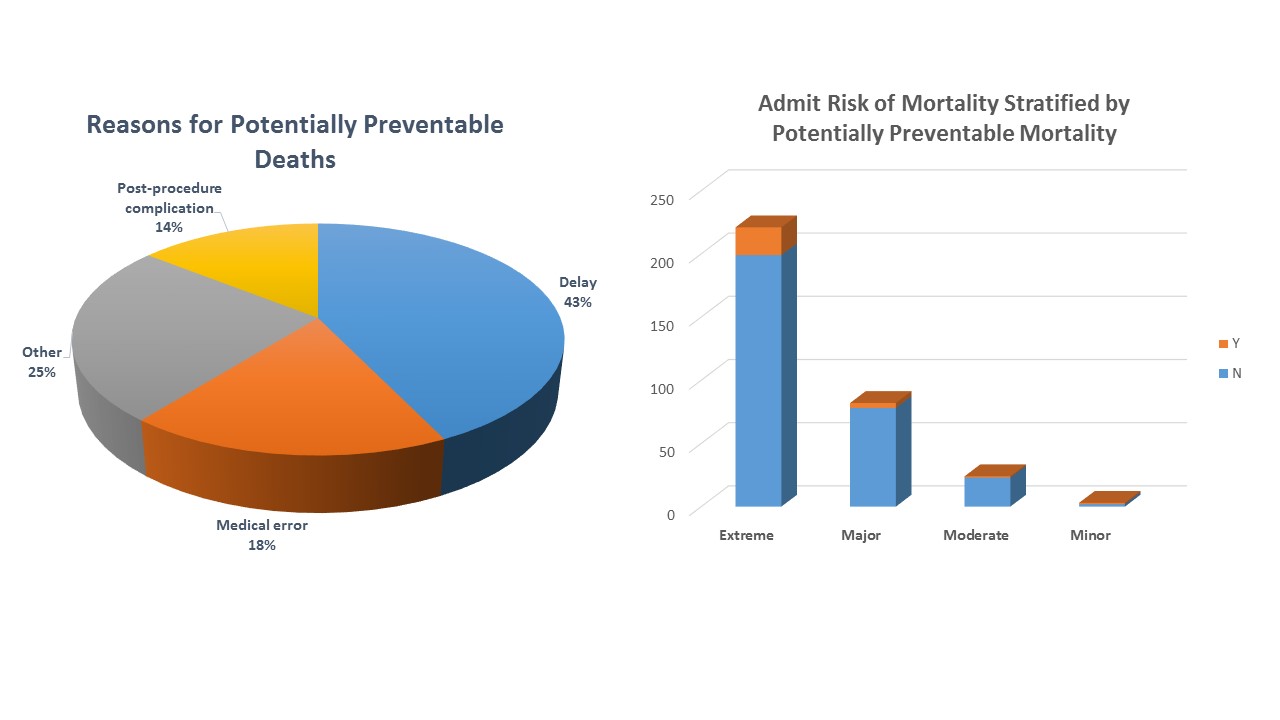
Results: A total of 330 mortalities were identified, of which about one half were female (47.6%). The average age at the time of death was 68. Transplant patients accounted for 14.8% of the sample. Nearly three quarters of the deaths occurred in the intensive care units, and 74.5% were on comfort care. The relative expected mortality according to the APR-DRG was “extreme” in 67.0% and “major” in 24.8% of patients. The causes of death were diverse, although infection was the most frequent culprit (52.1%). About 8.4% of cases had a degree of preventability, although very few were probably preventable (2.4%). The Cohen’s kappa for inter-observer reliability was 0.267. Delays were the most common reason for potentially preventable mortality, accounting for 42.9% of potentially preventable deaths. Examples include delay in administering antibiotics for sepsis, delay in paracentesis in those with cirrhosis, and delay in diagnostic radiologic studies such as a CT angiography chest to evaluate for an aortic dissection. The remainder of etiologies were divided between medical errors (17.9%), post-procedural complications (14.3%), and other errors (25.0%). Medical errors included inadequate antibiotic coverage and incorrect dosing of blood thinners. About 93% of deaths that were deemed potentially preventable had an extreme or major risk of mortality on admission.
Conclusions: Our inpatient population was incredibly complex with a high admission risk for mortality. Approximately 8% of cases were judged to have a degree of preventability, although most were not likely preventable. Delays in care were the most frequent reasons for potential preventability. Preventable mortality is difficult to study given its subjectivity but is an important tool for developing targeted quality improvement initiatives.