Background: Direct-care hospitalist teaching services (DCHTS), in which medical students rotate directly with hospital medicine faculty, have increased substantially. National data show that while only 9% of students rotated in this model in 2010 (1), by 2019, 45% of medical centers had adopted it, with another 25% considering implementation (2). These rotations emerged to address reduced availability of traditional teaching teams (TTTM) and rising learner volumes across specialties. Despite its growth, DCHTS presents challenges. Faculty on this rotation report higher stress and burnout, citing time management difficulties and unclear expectations. Acting as both primary physician and sole educator, these attendings struggle to balance patient care responsibilities with teaching, evaluation, and feedback. Students’ experiences are also mixed, with some reporting that they felt like “burdens” in this model. Nonetheless, this rotation offers unique opportunities: students observe real-time clinical workflows and decision-making and a learning environment akin to an apprenticeship. However, without structured support, the challenges can seem daunting . Our institutions aimed to leverage DCAM’s strengths through a standardized curriculum emphasizing a weekly focus on specific Entrustable Professional Activities (EPAs), structured feedback tools, clinical reasoning teaching material, and transparent scheduling.
Purpose: We created a structured Direct Care Apprenticeship Model (DCAM) curriculum to transform DCHTS into a sustainable, high-value rotation that supports faculty and improves the student learning experience.
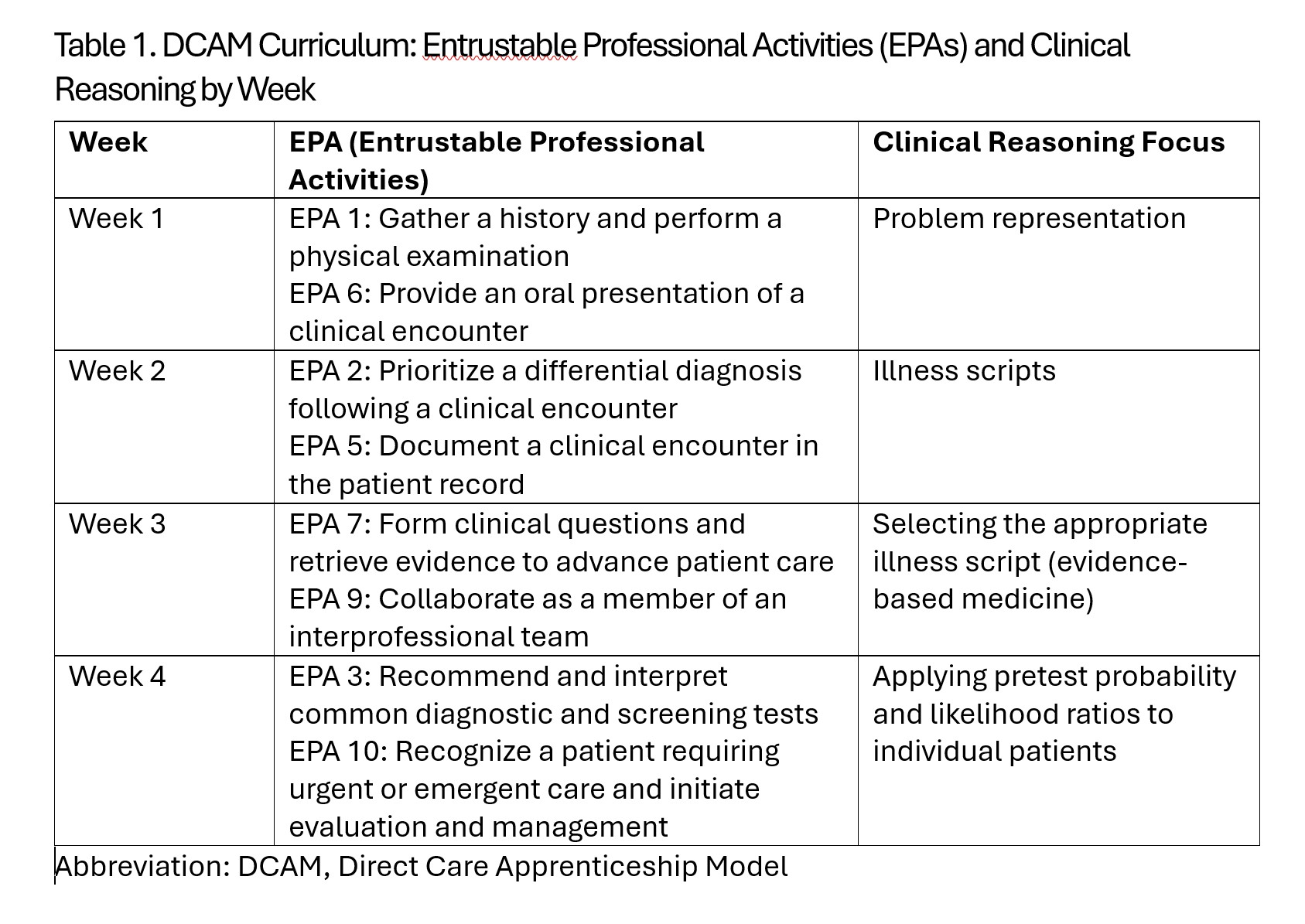
Description: We conducted quantitative and qualitative baseline assessments of faculty and students regarding attitudes toward DCHTS. We then developed a DCAM curriculum that spotlighted two EPAs and a clinical reasoning domain weekly (Table 1). To provide students with some structured independent learning and allow faculty time for independent work, teaching packets were created. These provided a more in-depth look at that clinical reasoning domain and could be used during the independent study time. Additionally, we provided a standardized schedule at each institution. Finally, we created an educational handoff tool (Figure 1). This served multiple purposes: (a) it allowed students a tool for self-evaluation; (b) faculty had a means of both providing structured feedback to the student; (c) the tool created a shared mental model between the off-going and oncoming attending, and (d) the form could be used to create the summative evaluation. We provided faculty development prior to the onset of the curriculum intervention and then implemented the curriculum. Curriculum use on the rotation was encouraged but not mandatory. We followed this with quantitative and qualitative assessments of students and faculty. Currently, a complete analysis of this data is in progress. However, preliminary results indicate that the curriculum was impactful, even though curricular uptake was inconsistent, remaining limited by clinical demands.
Conclusions: DCAM curriculum demonstrated promise in reducing faculty stress and enhancing student engagement on the DCHTS service with structured learning and feedback tools. While preliminary results suggest positive impact, consistent adoption remains a challenge due to competing clinical demands. Future endeavors to improve DCHTS should focus on intentional faculty support in this arena.
.jpg)