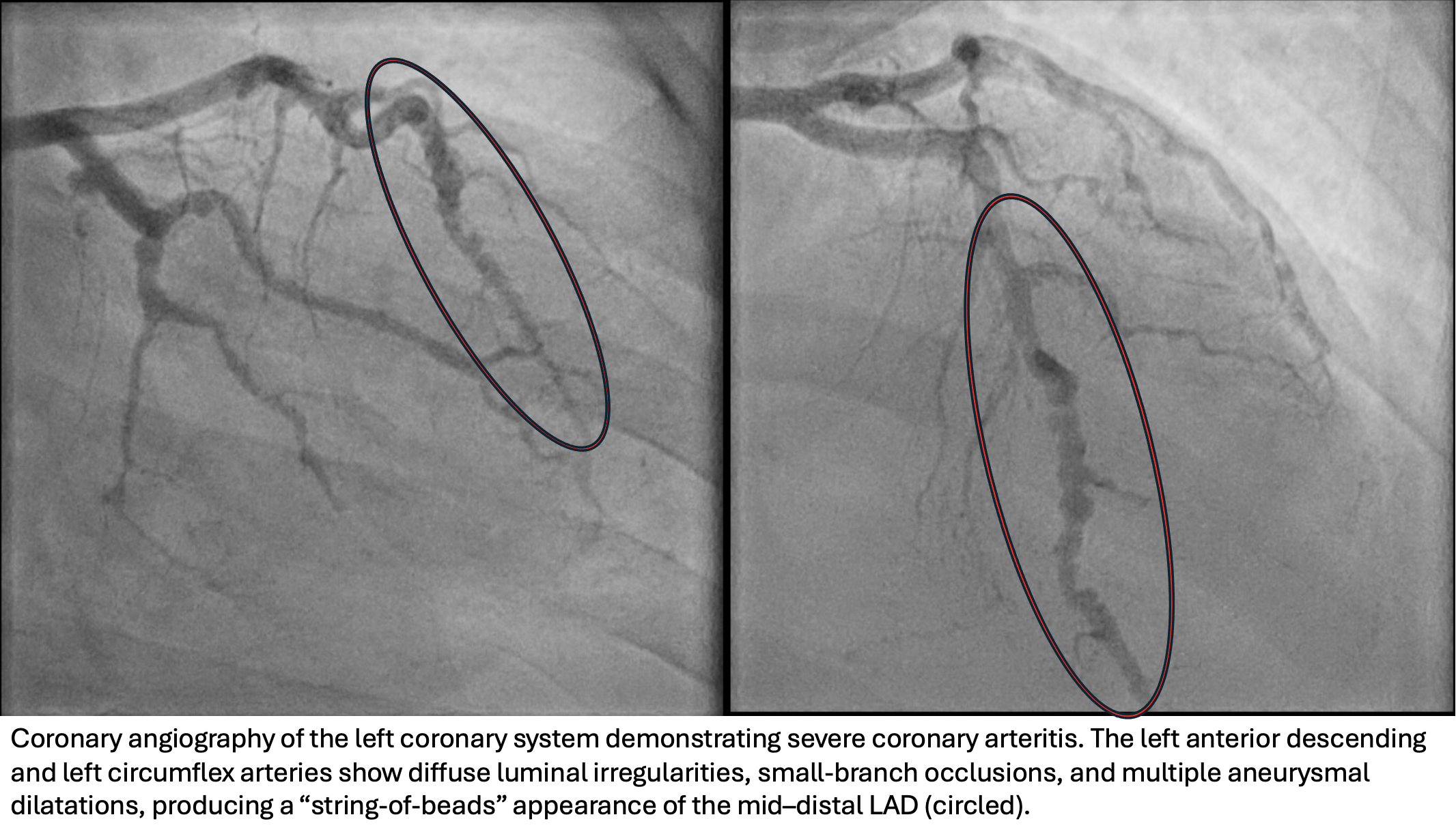
Case Presentation: A 24-year-old woman with recently diagnosed granulomatosis with polyangiitis (GPA), presented with worsening ocular pain and redness. Initial findings had included a 7.5 cm cavitary lung lesion, multiple pulmonary nodules, and leg lesions consistent with pyoderma gangrenosum (PG). She was c-ANCA positive, and bronchoscopy supported GPA. She was discharged on a steroid taper. During the taper, she developed anterior scleritis, prompting referral for inpatient re-escalation of immunosuppression. On arrival, she was tachycardic (~110 bpm) with mild erythema around PG lesions but no respiratory symptoms. Labs showed WBC 16.7 ×10⁹/L, CRP 145.8 mg/L, normal creatinine, and microscopic hematuria. Nephrology identified red cell casts on urine sediment. Pulse-dose steroids began to improve eye symptoms. On hospital day 4, she developed acute substernal chest pain seemingly relieved by position changes. ECG was normal, but troponin was >3000 ng/L; a previously drawn sample obtained before symptom onset was retrospectively found to be >2000 ng/L. Myopericarditis was suspected. Troponin peaked at >21,000 ng/L, and subsequent ECGs showed new lateral T-wave flattening despite resolution of pain. Echocardiogram revealed decreased apical contractility, and cardiac MRI showed a non-ischemic pattern of enhancement with diffuse hypokinesis, consistent with myocarditis. Coronary angiography subsequently demonstrated diffuse vasculitis affecting all three coronary territories, most pronounced in the mid-distal LAD, with several small-branch occlusions and aneurysms. MRA of the head, neck, abdomen, and pelvis showed no additional vascular involvement. She was treated with high-dose steroids, cyclophosphamide, avacopan, plasma exchange, and rituximab. Renal biopsy was deferred given clear evidence of active vasculitis. Medical therapy was prescribed to mitigate risk of accelerated coronary atherosclerosis.
Discussion: Cardiac manifestations—including pericarditis, myocarditis, coronary arteritis, and valvular disease—can occur across primary vasculidities, with variable frequency. Pericarditis is often managed conservatively, whereas myocarditis, coronary vasculitis, and valvular involvement typically necessitate urgent, aggressive treatment due to higher morbidity. Unrecognized or untreated heart involvement can yield poor prognosis.This patient developed a non–ST-elevation myocardial infarction due to coronary arteritis, confirmed by angiographic evidence of direct coronary involvement. GPA commonly targets small- and medium-sized vessels—predominantly affecting the kidneys, upper airways, and lungs—but can affect any organ system. Although long-term cardiovascular risk is elevated in GPA, clinically apparent coronary vasculitis remains rare. Subclinical myocardial involvement has been demonstrated to be more common and helps explain this patient’s elevated troponin levels prior to symptom onset. Management requires rapid initiation of immunosuppression alongside standard cardiovascular risk reduction.
Conclusions: Coronary arteritis is an uncommon but serious manifestation of GPA and can precipitate myocardial infarction even in the absence of traditional cardiovascular risk factors. Clinicians should maintain a high index of suspicion for cardiac involvement when evaluating GPA flares. Early diagnosis and treatment are essential to reduce morbidity and long-term mortality.