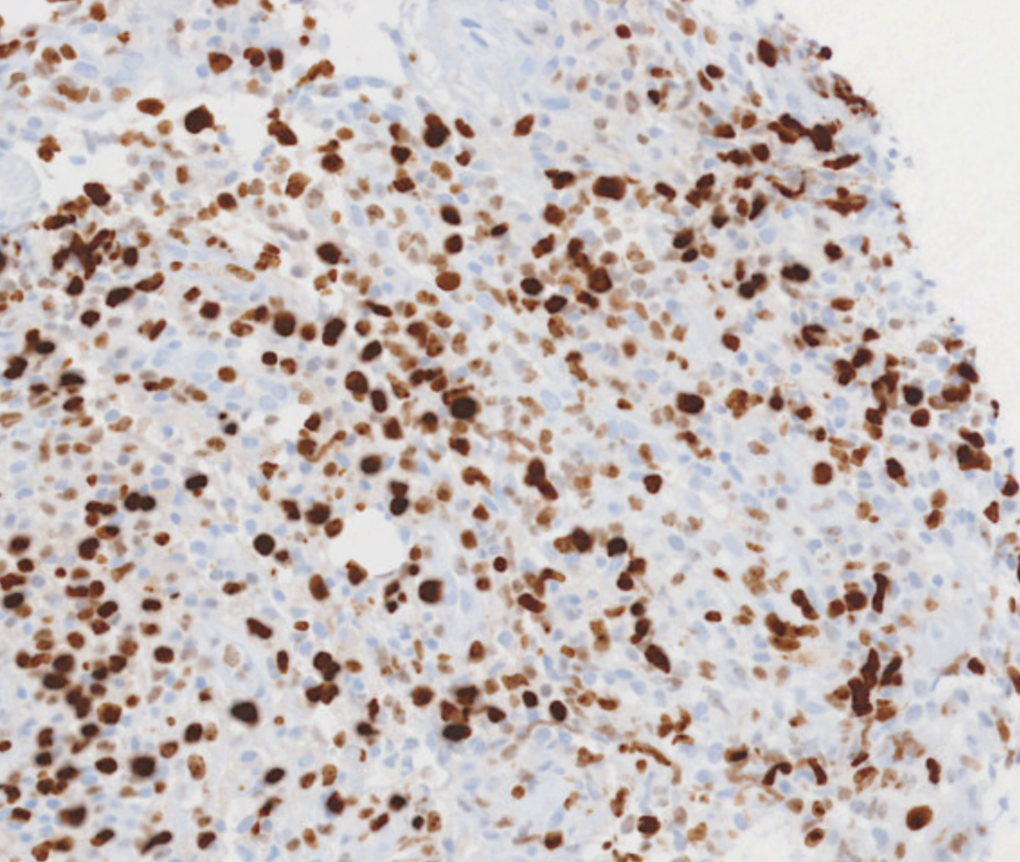
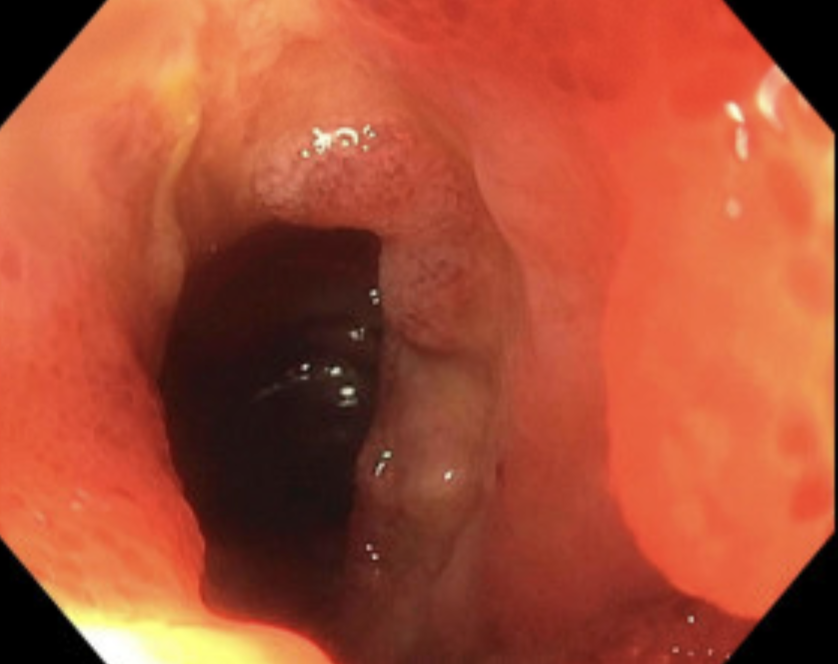
Case Presentation: An 80-year-old male with high-grade myelodysplastic syndrome (MDS) on chemotherapy and chronic transfusion dependence presented with neutropenic fever and hematochezia for three days. His past medical history included recent hospitalization for gastrointestinal bleeding with endoscopic and capsule evaluation showing diffuse nonbleeding ileal ulceration and biopsy-confirmed nonspecific pseudopyloric metaplasia. On presentation, he was tachycardic and pancytopenic (ANC 260/uL, hemoglobin 5.9 g/dL, platelets 2 x10*3/µL), requiring urgent transfusions. CT angiography of the abdomen and pelvis showed no active bleeding. Urgent colonoscopy revealed diffuse terminal ileal ulceration and scattered discrete colonic ulcers. Initial biopsy results were nondiagnostic, including negative CMV stain and no evidence of vasculitis or lymphoma. His course was complicated by persistent neutropenic fevers despite antibiotics and daily platelet transfusions. Repeat peripheral flow cytometry showed rising CD34+ myeloblasts with aberrant immunophenotype, expanded monocytic elements, and decreased maturing granulocytes concerning for malignant transformation. Sigmoidoscopy was repeated for additional biopsy sampling. Extensive histopathological analysis revealed myeloid sarcoma. The patient declined repeat bone marrow biopsy to further assess leukemic burden or transformation to acute myeloid leukemia. A family meeting was held, and he transitioned to comfort care. He passed away peacefully.
Discussion: This case highlights a rare cause of gastrointestinal bleeding in patients with high-grade MDS. The differential initially included inflammatory bowel disease causing severe bleeding in the setting of thrombocytopenia, infectious colitis, and MDS-associated Behcet syndrome. Persistent symptoms and nondiagnostic biopsies prompted repeat tissue sampling, which revealed diffuse ileal and colonic ulcers consistent with myeloid sarcoma. Although transformation to acute myeloid leukemia (AML) is an indicator of progression in MDS, a less common manifestation is myeloid sarcoma—an extramedullary proliferation of myeloid blast cells disrupting tissue architecture, essentially the tissue equivalent of AML. Myeloid sarcoma can affect any body part, more commonly skin, lymph nodes, and the urogenital system; gastrointestinal involvement is rare but associated with bleeding, perforation, necrosis, and obstruction. Outcomes are poor, even with intensive AML-type chemotherapy or stem cell transplantation.
Conclusions: We present a case of myeloid sarcoma as a rare yet clinically significant extramedullary manifestation of progression in high-risk MDS. Gastrointestinal involvement is particularly uncommon and mimics conditions like infectious colitis or inflammatory bowel disease. In MDS patients with gastrointestinal symptoms and rising peripheral blasts, extramedullary transformation should be considered, and repeat biopsy pursued when initial pathology is inconclusive. Early recognition facilitates expert consultation and timely goals of care discussions.