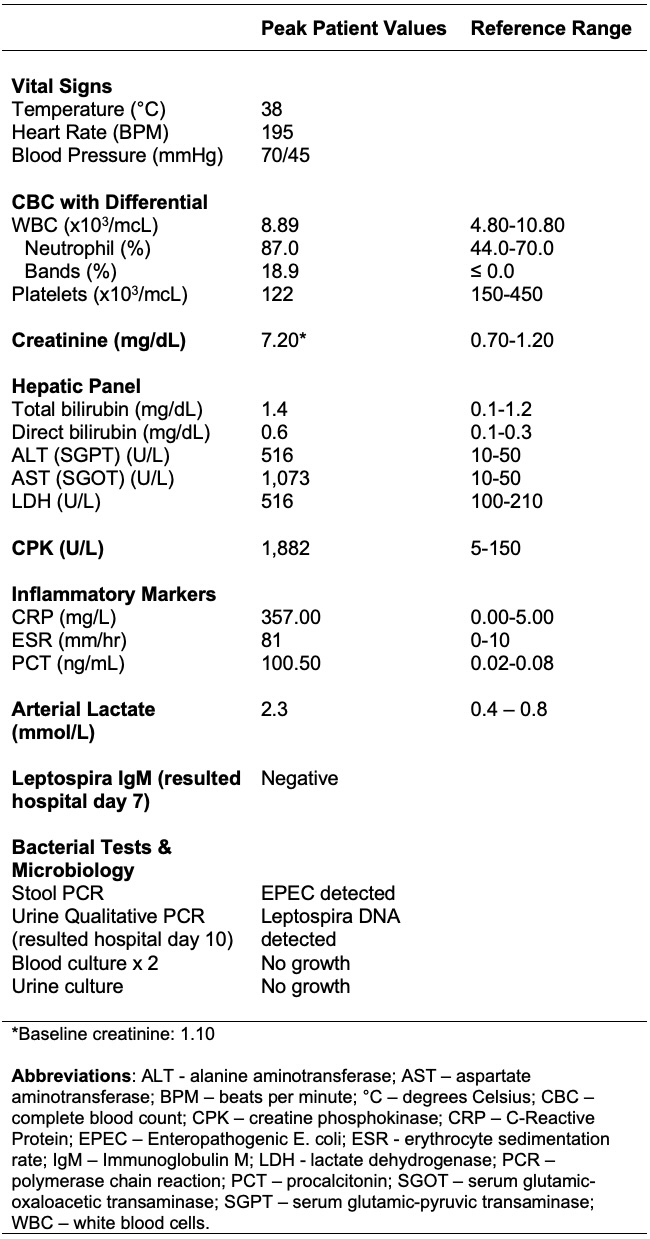
Case Presentation: A 55-year-old male with a history of hypertension and diabetes mellitus presented with fatigue, myalgias, vomiting, and diarrhea for two days. He worked as a grocery clerk in New York City and reported no recent recreational water activities or international travel. On physical exam, he was febrile, tachycardic, and hypotensive with bilateral calf tenderness. He did not have scleral icterus, conjunctival suffusion, or abdominal tenderness. Notable labs are reported in table 1. Stool PCR detected Enteropathogenic E. coli (EPEC). His EKG demonstrated atrial fibrillation with rapid ventricular response. He was admitted to the cardiac care unit for vasopressor administration and management of atrial fibrillation. He was treated for septic shock on hospital day 1 with empiric piperacillin-tazobactam and azithromycin to target EPEC. A 7-day course of doxycycline, a first-line agent for leptospirosis, was empirically initiated on day 5. His diarrhea resolved, hepatorenal injury and rhabdomyolysis improved, and vasopressors were discontinued prior to initiating doxycycline. He spontaneously converted to normal sinus rhythm and was transferred to the general wards within two days of doxycycline initiation. Leptospira tests collected on day 2 resulted after doxycycline initiation. Immunoblot was negative for IgM antibodies but qualitative urine PCR detected leptospira DNA. At a one-week follow-up visit, he did not have residual symptoms, his hepatic injury resolved, and his creatinine continued to trend down toward his baseline.
Discussion: Leptospirosis is the most common spirochetal zoonotic infection globally and is predominantly endemic in tropical regions. Although less than 0.1% of incident cases are identified in the U.S.1, its prevalence is increasing due to rising temperatures and more extreme weather events caused by climate change2. Transmission occurs through contact with infected animals—particularly rodents—or their urine, often through occupational exposures or contaminated water sources. Our patient’s infection despite the lack of occupational exposure or travel to an endemic region underlines the importance of residence in crowded urban settings as a key underrecognized exposure in the U.S.3Leptospirosis has a spectrum of clinical presentations ranging from a mild flu-like illness to rapidly progressive multisystem dysfunction1. As laboratory diagnostics often require send-out testing, providers must remain vigilant to the clinical features that suggest this infection and initiate treatment before confirmatory testing is available. Although the patient’s presentation was in part explained by his infection with EPEC, the unique combination of a febrile diarrheal illness that presented with myalgias, hyperbilirubinemia, thrombocytopenia, hepatorenal injury, and rhabdomyolysis led to appropriate testing for and empiric treatment of leptospirosis. It is important to maintain a high index of suspicion for leptospirosis despite negative serological testing given the limited sensitivity of these assays early in the disease course4–6.
Conclusions: Individuals residing in crowded urban settings are at risk of contracting leptospirosis even in non-endemic countries. Given its high morbidity and mortality without treatment, hospitalists practicing in these settings should consider empiric treatment of leptospirosis in patients with severe presentations of acute febrile illnesses with consistent features while awaiting laboratory confirmation.