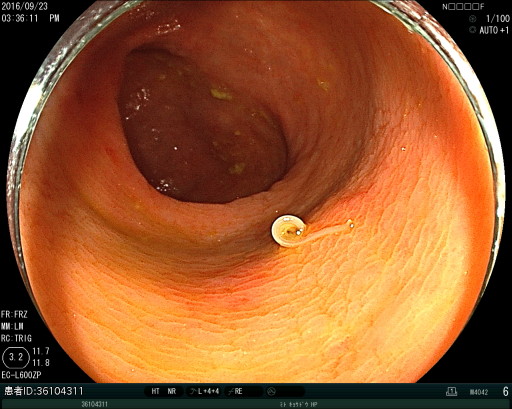
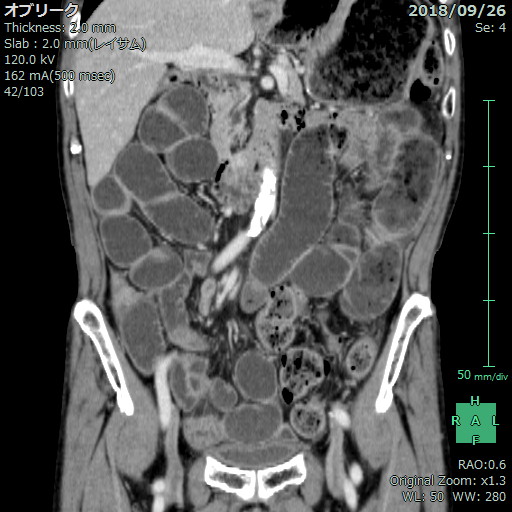
Case Presentation: 21 cases of small intestine anisakiasis were analyzed in terms of medical history, examinations of symptoms, vital signs, laboratory data, and CT findings. 9 cases were identified through specific anisakiasis Immunoglobulin E or Immunoglobulin A testing. 2 cases were confirmed by the detection of anisakis by endoscopic examination. 10 cases were diagnosed based on medical history and distinctive CT findings. All cases have a history of eating raw fish and abdominal pain for up to four days. Diarrhea and nausea were observed in 19% and 47.6% of cases, respectively. White blood cell and C-reactive protein levels were elevated in 67% and 90% of cases, respectively. The elevation of eosinophil was not significant. In the majority of cases, CT scans revealed ascites, extensive small intestinal dilation, mesenteric edema, bowel wall thickening, and fat stranding in the mesentery. These findings would normally suggest a need for emergency surgery but lack the distinctive whirl sign and torsion. Furthermore, all cases demonstrated an improvement in symptoms without resorting to surgical interventions. The average length of stay was 4.4 days. No cases required narcotic analgesic and were treated with acetaminophen for the pain.
Discussion: Anisakiasis is a rare parasitic gastrointestinal disease caused by eating raw or undercooked fish. While most cases are gastric manifestations and necessitate endoscopic therapy, small intestinal anisakiasis comprises a mere 2.5% of cases. Small intestinal anisakiasis may be treated conservatively without invasive surgical procedures; however, case reports indicate that diagnostic surgery is often performed anyway due to severe CT findings. The main cause of intestinal obstruction was localized intestinal wall edema. In addition to the food consumption history of the patient, factors such as extensive intestinal edema, ascites, and bowel wall thickening without torsion may be key to diagnosis. Given that anisakiasis takes 4 days to develop in our cases and raw fish consumption is more commonplace in certain countries compared to others, travel history may also be taken into consideration.
Conclusions: In conclusion, small intestinal anisakiasis may be possible to diagnose based on the history of eating raw fish and CT findings, and may be treated conservatively. This case series contributes to the clinical findings of anisakiasis and the efficacy of conservative treatment, and to illuminate the need to prevent urgent surgical procedures for diagnosis.