Background: Prolonged lengths of stay (PLOS) on general internal medicine wards are associated with increased mortality and morbidity for patients and represent a costly source of health care spending [1]. Increasingly, nonmedical barriers to discharge, including the need for guardianship, limited facility options, and lack of home support are recognized as contributors to PLOS in the U.S. However, few studies in the last decade have examined this association [2]. This study aims to expand upon previous work in the field by reviewing in greater detail the nonmedical factors associated with PLOS in the U.S. in a general internal medicine patient population.
Methods: We conducted a retrospective chart review of all patients admitted from 1/1/2018 -12/31/2019 with PLOS who were discharged from a general medicine floor of our urban academic teaching hospital. PLOS was defined as lengths of stay greater than or equal to 30 days [3]. We collected demographic, clinical, and administrative data for each admission. Through review of medical and care coordination notes, we examined barriers to discharge at lengths of stay of 30 days, 60 days, and 90 days. Barriers were defined as “medical” if patients were not medically ready for discharge and “nonmedical” when patients who were medically ready for discharge stayed inpatient. Nonmedical barriers were further divided into subcategories of (1) discharge planning and (2) awaiting placement, within which descriptions of the specific delay were recorded based on taxonomy of previous studies [4, 5]. In cases with more than one nonmedical barrier, multiple barriers were noted. Descriptive analyses were conducted on the data.
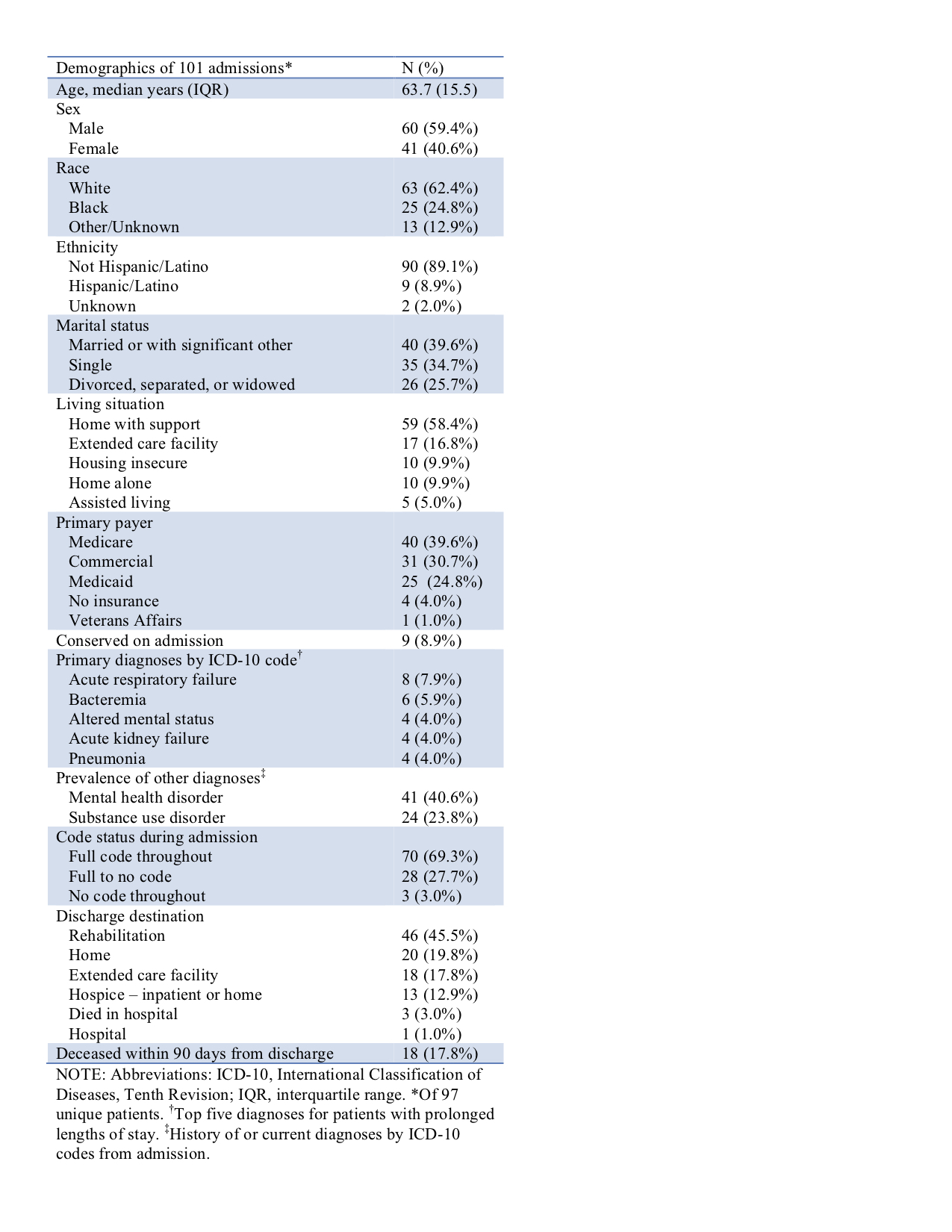
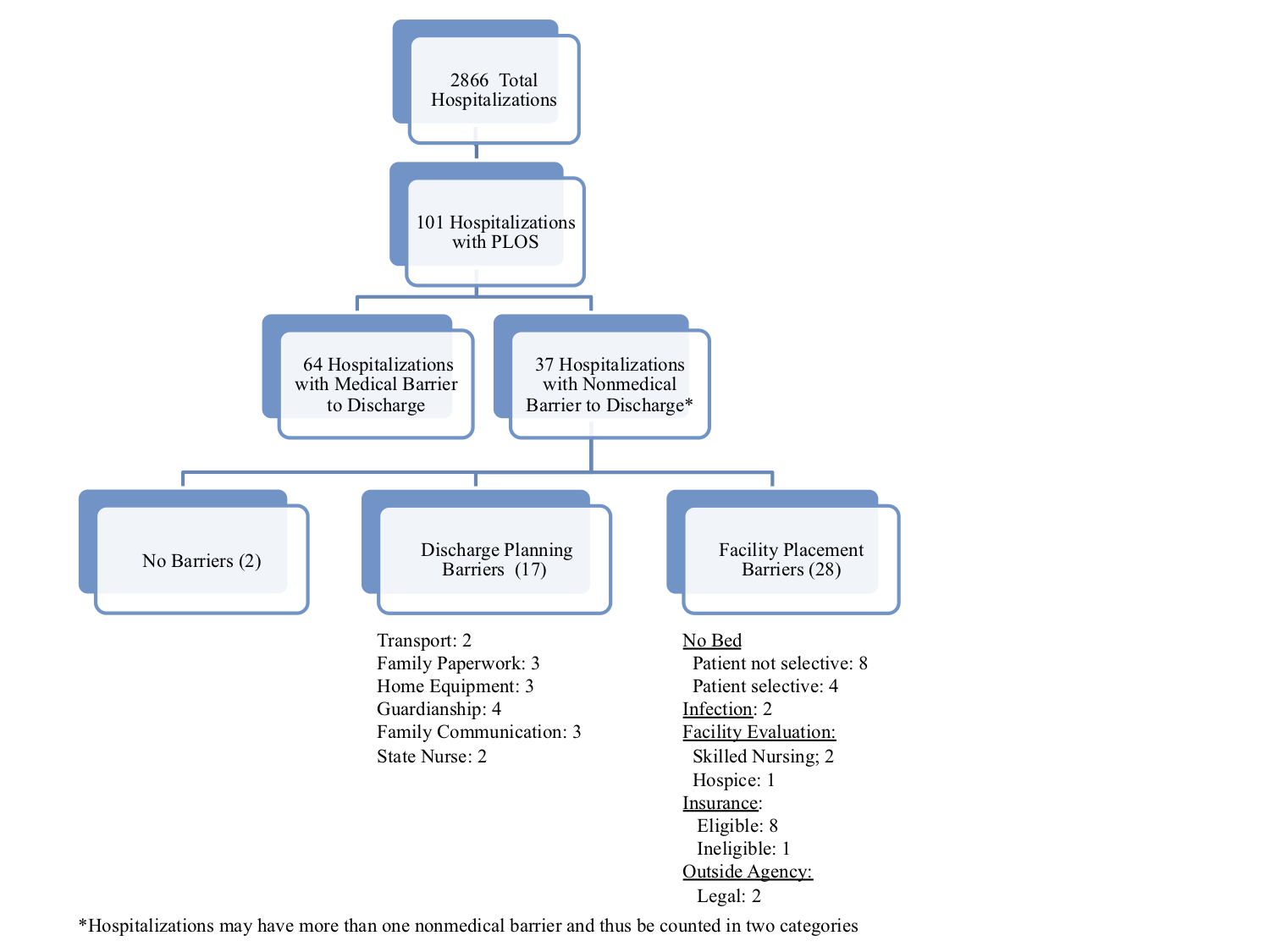
Results: Of 2866 hospitalizations, 101 hospitalizations (3.5%) of 97 patients (see table 1 for demographics) were found to have PLOS. PLOS accounted for a total of 6518 (27.2%) of 23,934 inpatient days. The median length of stay for the PLOS subgroup was 44.4 days (interquartile range: 38.2 days). Of 101 PLOS admissions, 37 hospitalizations lasted longer than 60 days, and 17 lasted longer than 90 days. At hospital day 30, 36.6% of hospitalizations with PLOS were found to have nonmedical barriers to discharge. At day 60, 59.5% of the 37 admissions were due to nonmedical barriers. Finally, at day 90, 52.9% of the remaining 17 admissions faced nonmedical barriers to discharge. The most common reason for a nonmedical stay at all three time points was barriers to facility placement, particularly facility rejections. Insurance coverage and awaiting communication with family regarding disposition were the second most common reason for nonmedical stays at 30 and 60 days, respectively. Of the 17 outliers with greater than 90 days length of stay, patient profiles and barriers to discharge varied with an age range of 33.5 to 80.9 years. Of note, barriers to discharge changed over time, with five hospitalizations with nonmedical barriers then evolving into medical barriers by the next time point and 16 hospitalizations switching from medical to nonmedical delays.
Conclusions: PLOS in a small proportion of patients contribute to a disproportionately high number of total inpatient days. Nonmedical factors contribute to approximately one third of PLOS cases at 30 days and more than half of cases beyond 60 days in our sample. The rising prevalence of nonmedical barriers, particularly the lack of facility bed offers, underscores the need to further study the impact of these delays on patients, health care providers and hospitals.