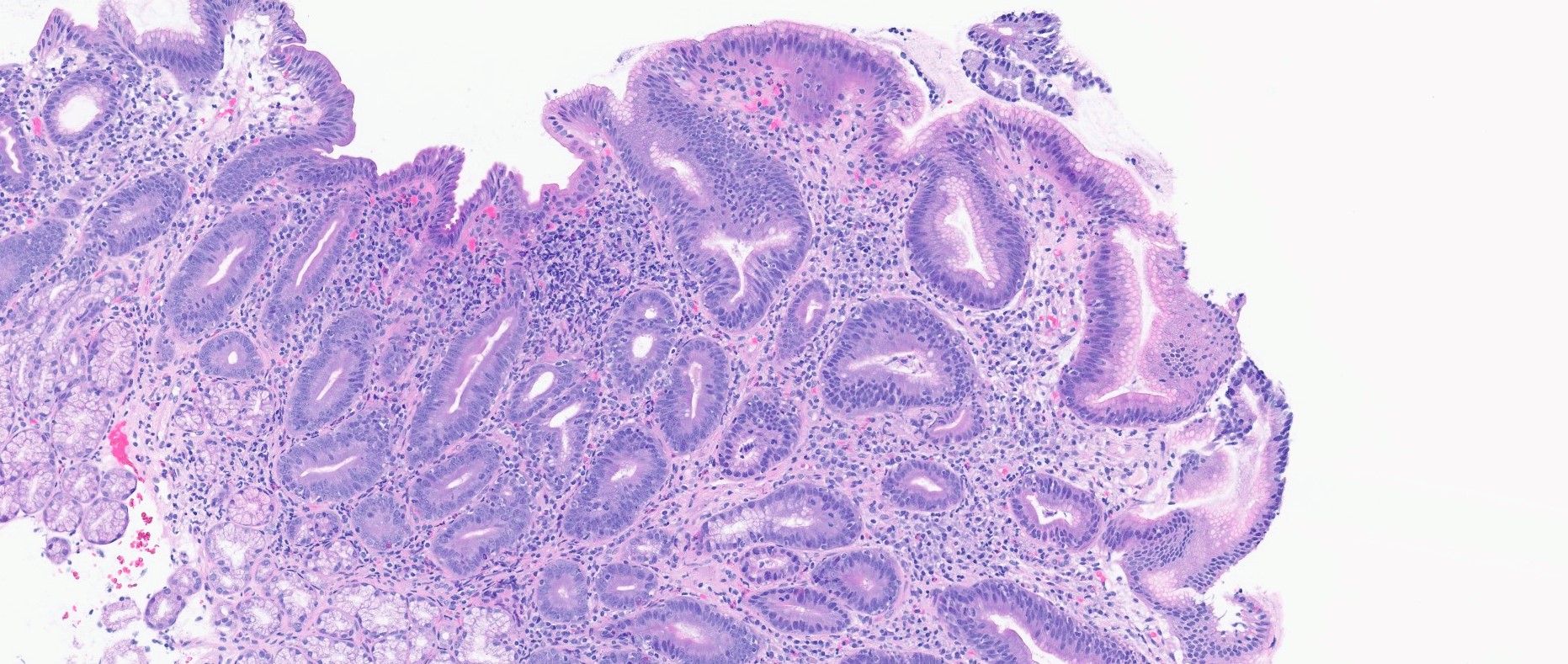
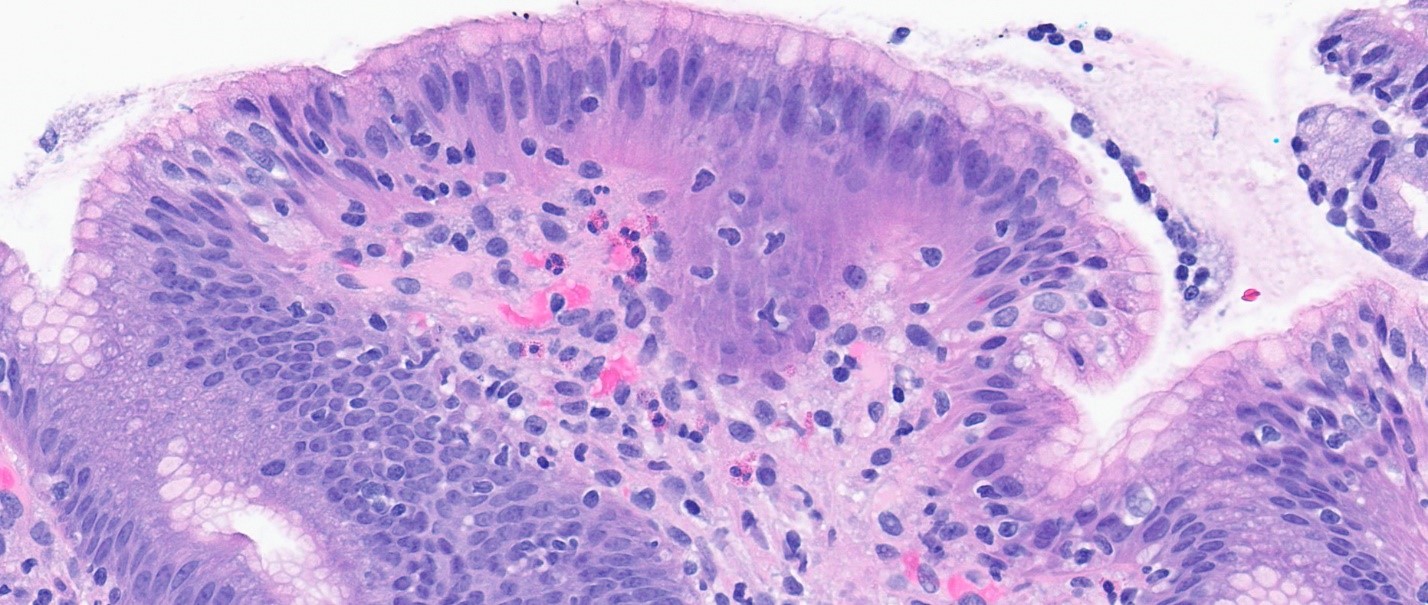
Case Presentation: A 75-year-old woman with hypertension presented to the emergency department with months of progressive diarrhea. She reported a 9-month history of non-bloody loose stools, which fluctuated from one to ten episodes per day, and resulted in an unintentional 40-pound weight loss.Outpatient evaluation included negative Clostridioides difficile toxin, gastrointestinal pathogen panel, and ova and parasite assays. She had a normal thyroid-stimulating hormone, chest computed tomography (CT), and mammogram. Esophagogastroduodenoscopy (EGD) revealed normal esophagus, stomach, and duodenum. Gastric biopsies showed chronic gastritis with lymphoplasmacytic infiltrate and was negative for Helicobacter pylori, metaplasia, and dysplasia. Duodenal biopsies demonstrated villous blunting with intraepithelial neutrophilic and lymphocytic infiltrates. Cytomegalovirus and Giardia stains were negative. Colonoscopy showed a 4 mm hyperplastic transverse colon polyp and diverticulosis. Celiac serologies were negative. Empiric treatment with doxycycline for Small Intestinal Bacterial Overgrowth (SIBO) did not resolve symptoms.On admission, she was hypotensive. Labs were notable for creatinine 5.01 mg/dL (baseline of 1.2 mg/dL), chloride 121 mmol/L, bicarbonate 15 mmol/L, erythrocyte sedimentation rate 35 mm/h, and C-reactive protein < 5 mg/L. Infectious stool studies were again negative. Stool osmotic gap was 69. CT of the abdomen demonstrated acute colonic diverticulosis with inflamed diverticulum in the sigmoid colon, possibly representing uncomplicated acute diverticulitis. She received fluid resuscitation with subsequent improvement in acute kidney injury and metabolic derangements. She was treated with ciprofloxacin and metronidazole for diverticulitis; however, her diarrhea persisted. Repeat EGD and duodenal biopsies demonstrated severe villous blunting and intraepithelial lymphocytosis (Figures 1 and 2 respectively). These histologic findings, while nonspecific, were compatible with olmesartan-induced enteropathy (1). Repeat colonoscopy was deferred in the setting of acute diverticulitis. Olmesartan was discontinued during her hospitalization and she was initiated on anti-diarrheal medications. The patient’s diarrhea improved markedly within days, and at outpatient follow-up two months after discharge, her diarrhea had fully resolved without any need for further anti-diarrheal medications.
Discussion: Olmesartan-induced enteropathy is an underdiagnosed etiology of chronic non-bloody diarrhea that can occur in individuals who have been taking olmesartan for months to years (2-6). Other symptoms include nausea, vomiting, abdominal pain, bloating, weight loss, and fatigue (3-5). Intestinal biopsies often show sprue-like enteropathy findings in the duodenum, such as villous atrophy and varying degrees of intraepithelial lymphocytosis with or without subepithelial collagen deposition (2-6). Infectious and malabsorptive workup are unrevealing, although Human Leukocyte Antigen DQ2/DQ8 has been associated with this condition (3,6). SIBO can co-occur, but antibiotics do not resolve the diarrhea (3). After cessation of olmesartan, patients can experience symptomatic improvement within weeks and histological remission within months (3,5).
Conclusions: Clinicians should have a high degree of suspicion for olmesartan-induced enteropathy in patients with persistent diarrhea despite negative infectious and celiac testing.