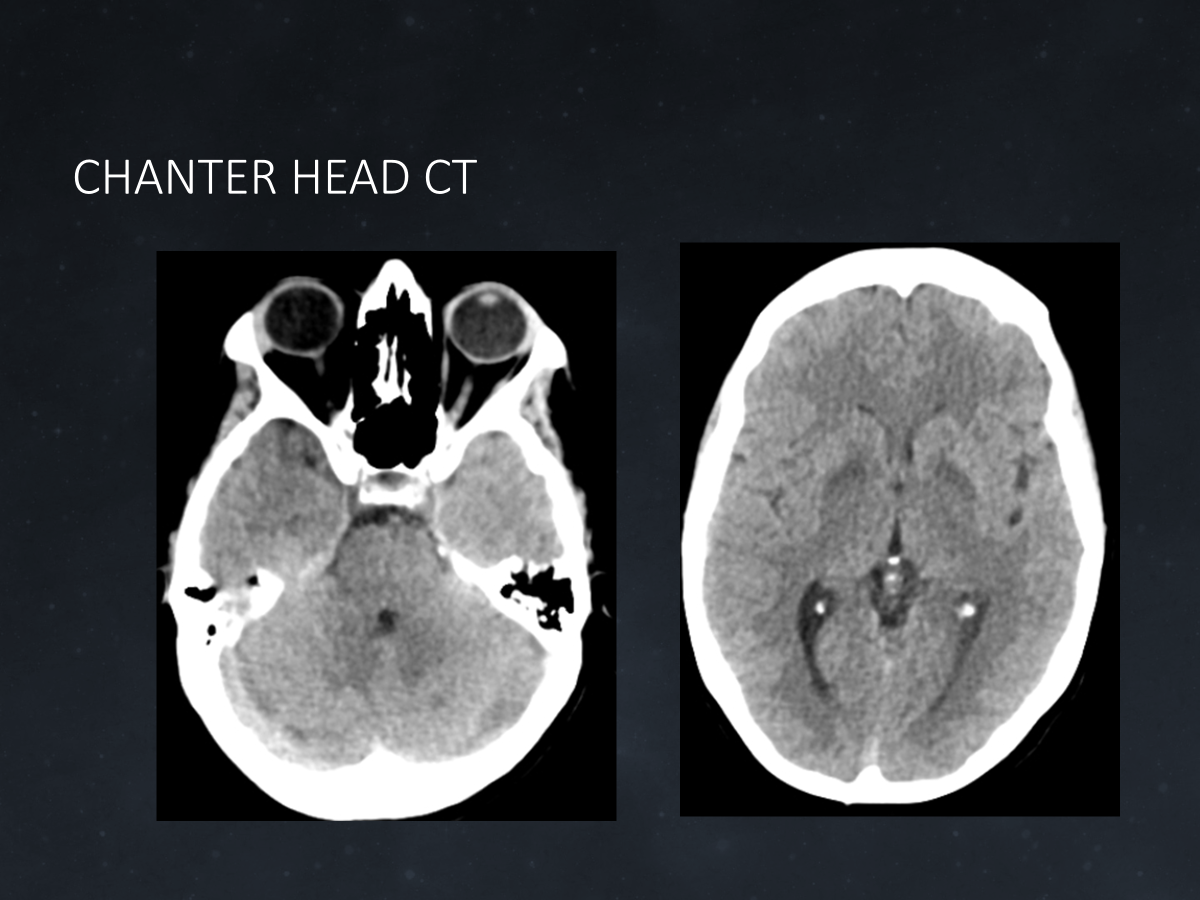
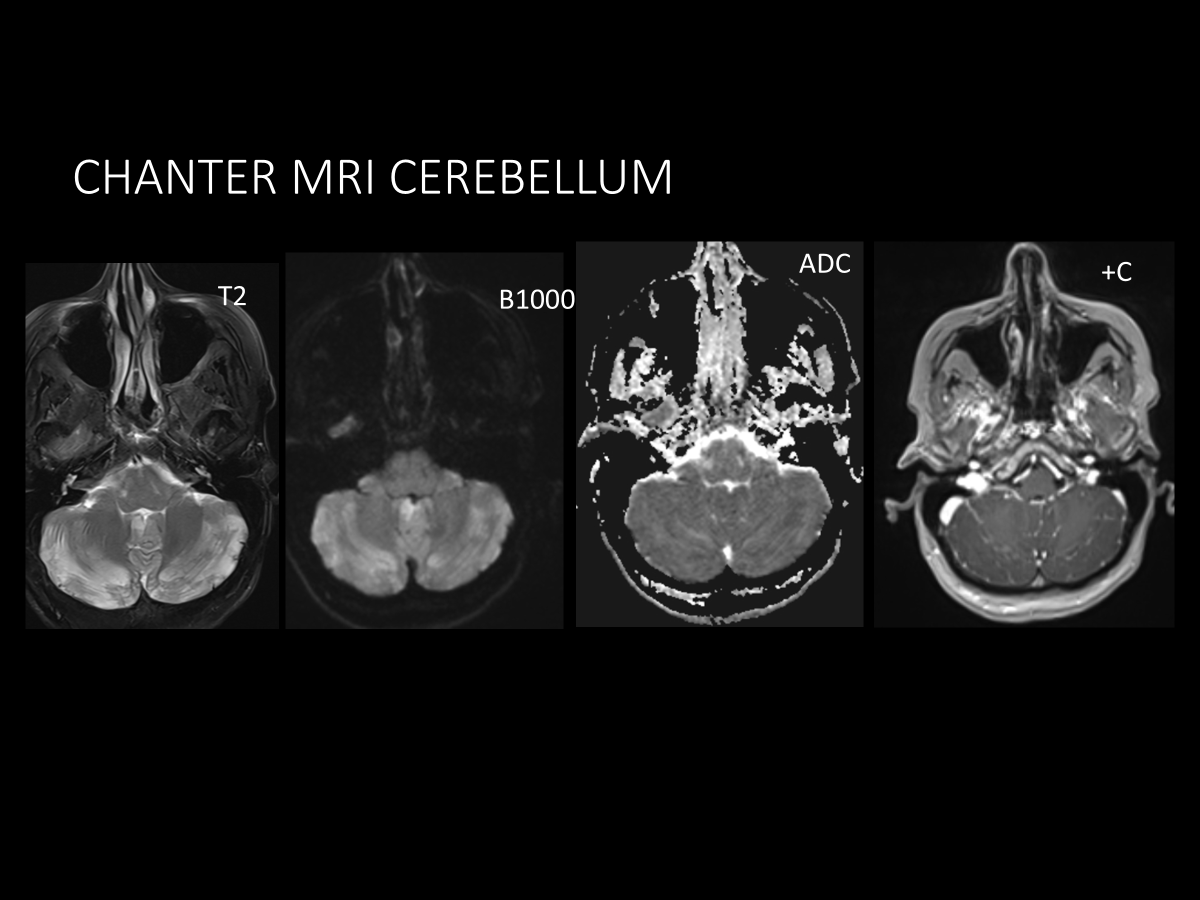
Case Presentation: A 49-year-old female presented with confusion. Her family reported possible intravenous drug use, but she had no memory of preceding events. She was unable to form new memories. Review of systems was normal but limited by recall. She was afebrile, normotensive, not tachycardic, and saturating well on room air. Heart rhythm was regular, lungs were clear, and there was no neck stiffness. She had mild suprapubic tenderness. Patient was only oriented to self. Cranial nerves, motor, sensory, and coordination were normal. Urine drug screen was positive for amphetamines and fentanyl. Laboratory studies showed elevated liver enzymes without leukocytosis and normal electrolytes and renal function. Urinalysis was consistent with urinary tract infection, and ceftriaxone was started. Hepatitis C was later confirmed as the cause of her transaminitis. Extensive infectious, metabolic, toxic, and inflammatory studies of the serum and cerebrospinal fluid were otherwise normal. Head computed tomography revealed parenchymal hypodensities in the basal ganglia and cerebellum (Figure 1), concerning for toxic-metabolic encephalopathy (TME). She was managed expectantly for TME until magnetic resonance imaging (MRI) revealed focal restricted diffusion in the cerebellum/dentate nuclei (Figure 2), globus pallidus, caudate, and hippocampi. These findings, along with her persistent retrograde and anterograde amnesia and fentanyl exposure, were most consistent with Cerebellar-Hippocampal-Basal Nuclei with Restricted Diffusion (CHANTER) syndrome. Her condition improved slightly with cognitive rehabilitation, including structured memory tools, but her amnestic deficits persisted. Neurology, physical therapy, occupational therapy, speech therapy, and case management were engaged to coordinate rehabilitation and a safe discharge plan to a rehabilitation facility.
Discussion: CHANTER syndrome, first described in 2019, is a rare neurotoxic encephalopathy most often associated with opioid toxicity. Patients present with altered mental status, ranging from minimal responsiveness and disorientation to profound anterograde and retrograde amnesia. CHANTER can be difficult to distinguish from other common causes of altered mentation and amnesia, including stroke, trauma, psychogenic, seizure, infection, substances, toxins, and medications. However, the MRI pattern seen in CHANTER, restricted diffusion and edema in the cerebellum, hippocampus, and basal ganglia, is distinct. With rising recreational opioid use, hospital physicians are likely to encounter more patients with CHANTER, making a high index of suspicion and early MRI essential.
Conclusions: Without formal diagnostic guidelines for hospitalists, a suggested clinical dyad for CHANTER includes: (1) documented fentanyl or other opioid exposure, and (2) clinical presentation with altered mental status and/or amnesia. These findings should prompt consideration of early MRI, especially if the initial CT is abnormal. Early recognition of CHANTER is essential to enable prompt diagnosis, timely neurologic monitoring, and impactful supportive care. A multidisciplinary approach with social work, addiction medicine, and therapy services is critical to optimize recovery and address substance use disorder. Prognosis is generally favorable if patients abstain from the offending agent, underscoring the importance of sustained treatment and structured follow-up care.