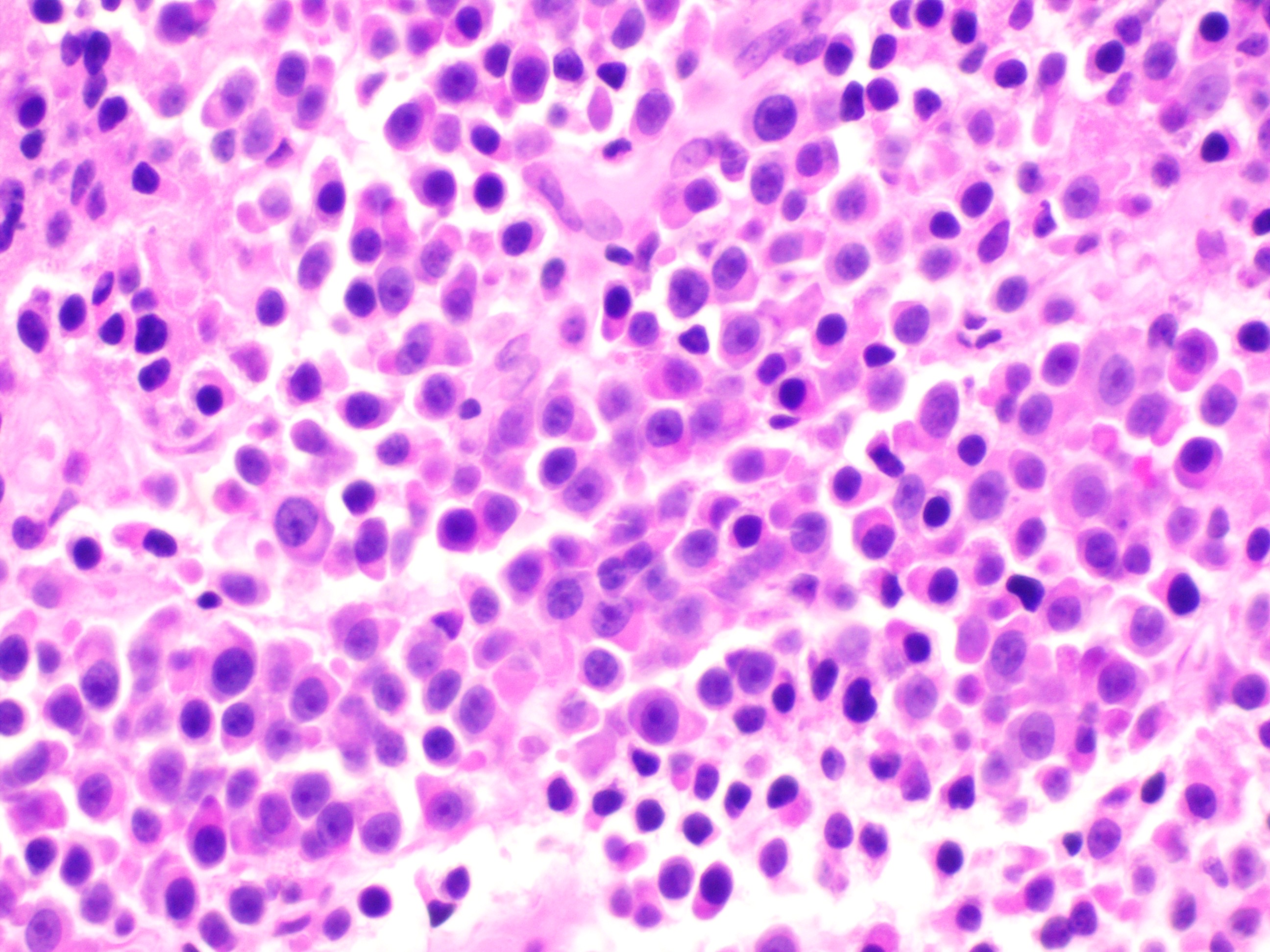
Case Presentation: A 71-year-old female with a history of ovarian cancer (status post chemotherapy and hysterectomy in 2016) presented with progressive dry cough and exertional dyspnea over three weeks, followed by nausea, vomiting, anorexia, fatigue, and a 20-pound unintentional weight loss over eight weeks. She denied hemoptysis.Initial labs revealed creatinine 5.2 mg/dL, phosphate 5.6 mg/dL, sodium 131 mmol/L, bicarbonate 17 mmol/L, and hemoglobin 6.9 g/dL. Infectious workup was negative. CA-125 was elevated at 80 U/mL. Chest CT showed a large pleural effusion, a mass encircling the right 6th rib, and a posterior mediastinal mass. Thoracentesis yielded atypical plasma cells. Serologic studies revealed a Kappa/Lambda ratio of 188.94, Beta-2-Microglobulin 0.22 mg/L, and IgG monoclonal spike of 7,330 mg/dL. Biopsy confirmed CD138+ plasma cells with kappa light chain restriction. Bone marrow biopsy showed 40–50% hypercellularity with 80–90% plasma cell infiltration, normal karyotype, and negative FISH and Congo red staining. Diagnosis: IgG Kappa Multiple Myeloma with plasmacytoma.Bone scan was negative for lytic lesions. Due to renal failure, the patient received two cycles of CyBorD (Bortezomib, Cyclophosphamide, Dexamethasone), complicated by Bortezomib-induced foot drop. MRI revealed lytic lesions at L4. With renal improvement (creatinine 2.54 mg/dL), therapy transitioned to D-VRd (Daratumumab, Bortezomib, Lenalidomide, Dexamethasone). The patient remained alive at three-month follow-up.
Discussion: Despite initial renal recovery, MPE portends poor prognosis due to selective elimination of proliferative clones. As an independent risk factor for relapse and progression, MPE warrants aggressive and innovative management. Emerging data suggest intrapleural Bortezomib may extend survival by up to seven months. This case reinforces the importance of early recognition and tailored therapy in MPE. This case is particularly important to the field of hospital medicine because Myelomatous Pleural Effusion (MPE), although rare, often presents first in the inpatient setting and requires hospitalists to make rapid, high-stakes clinical decisions. Hospitalists are uniquely positioned at the front line of recognizing atypical manifestations of common hematologic malignancies, especially when patients present with nonspecific symptoms such as dyspnea, renal failure, or pleural effusions.
Conclusions: MPE remains a rare but clinically significant manifestation of multiple myeloma. Vigilance in diagnosis and consideration of novel therapeutic approaches are critical to improving outcomes. This case contributes to the growing literature and highlights the need for further research into optimal management strategies.