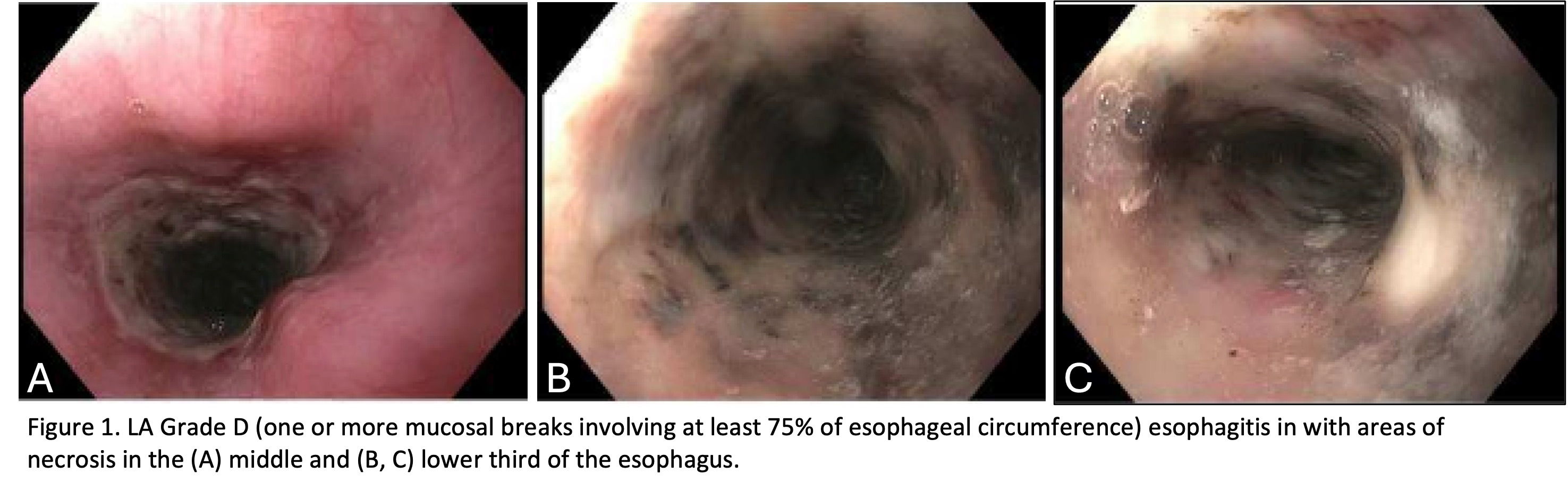
Case Presentation: A 73-year-old female with hypertension, chronic kidney disease (CKD), hyperlipidemia, type 2 diabetes, obesity, and hiatal hernia presented with 2 days of acute onset epigastric pain with associated nausea, non-bloody non-bilious vomiting, diarrhea, dysphagia, odynophagia, and inability to tolerate oral intake. She described the pain as constant and progressive. Her history included a 60 pack-year smoking history (quit 30 years ago) and no alcohol or drug use. Medications included insulin, apixaban, rosuvastatin, glipizide, semaglutide, and losartan.She was afebrile with normal vitals. Labs showed hyperglycemia (330 mg/dL), elevated creatinine (1.1 mg/dL, baseline ~1.2 mg/dL), transaminitis (AST 141 U/L, ALT 88 U/L), alkaline phosphatase (126 U/L), and lactate (1.9 mmol/L). Complete blood count, comprehensive metabolic panel, lipase, troponin, Clostridium difficile toxin, and gastrointestinal (GI) pathogen panel were unremarkable. CT abdomen/pelvis showed no acute pathology. She was admitted for supportive care. On hospital day 5, she developed melena with a hemoglobin drop (14 g/dL to 11 g/dL) and leukocytosis (12 x 109/L). Apixaban was held and IV pantoprazole started. EGD revealed 16 cm of circumferential necrotic esophagitis in the middle and lower third of the esophagus (Figure 1). Histology showed detached ulcer exudate and fibromuscular tissue with acute/chronic inflammation and focal granulation tissue. She was diagnosed with acute esophageal necrosis (AEN) and discharged on pantoprazole. Follow-up EGD one month later showed diffuse mucosal sloughing consistent with healing ischemic esophagitis. With persistent dysphagia and odynophagia, a subsequent repeat EGD one month later showed benign-appearing severe stenosis in the middle and lower esophagus. A gastric tube was placed for diversion and healing. The cause of her AEN remained unclear.
Discussion: AEN, or black esophagus, is a rare condition (prevalence of 0.01-0.02% of EGDs) defined by circumferential black mucosal discoloration of the distal esophagus with sharp demarcation at the gastroesophageal junction.(1-4) Pathogenesis is multifactorial, involving ischemia, impaired mucosal defenses, and corrosive injury from gastric reflux.(1, 3, 5, 6) Risk factors include advanced age, male sex, cardiovascular disease, diabetes, CKD, alcohol use, malnutrition, hypoalbuminemia, thromboembolic disease, malignancy, and hemodynamic compromise.(1-3, 6, 7) Typical symptoms are hematemesis, melena, epigastric pain, vomiting, and dysphagia.(1-3) Labs may show anemia and leukocytosis.(1) Diagnosis is made via EGD with the classic appearance as described. Histology may show mucosal/submucosal necrosis, thrombi, and pigment deposition, but biopsy is not required.(1, 4, 5) Management is supportive: IV fluids, hemodynamic stabilization, NPO status, and IV proton pump inhibitors.(1, 3, 4, 7, 8) Treating underlying causes is essential. Complications include perforation, mediastinitis, and strictures.(1, 3) Mortality is high (30–50%), usually due to comorbid conditions.(2-4)
Conclusions: Although rare, AEN should be considered in patients with upper GI bleeding and abdominal pain, especially those with known risk factors. Prompt recognition is essential to guide treatment and prevent serious complications.