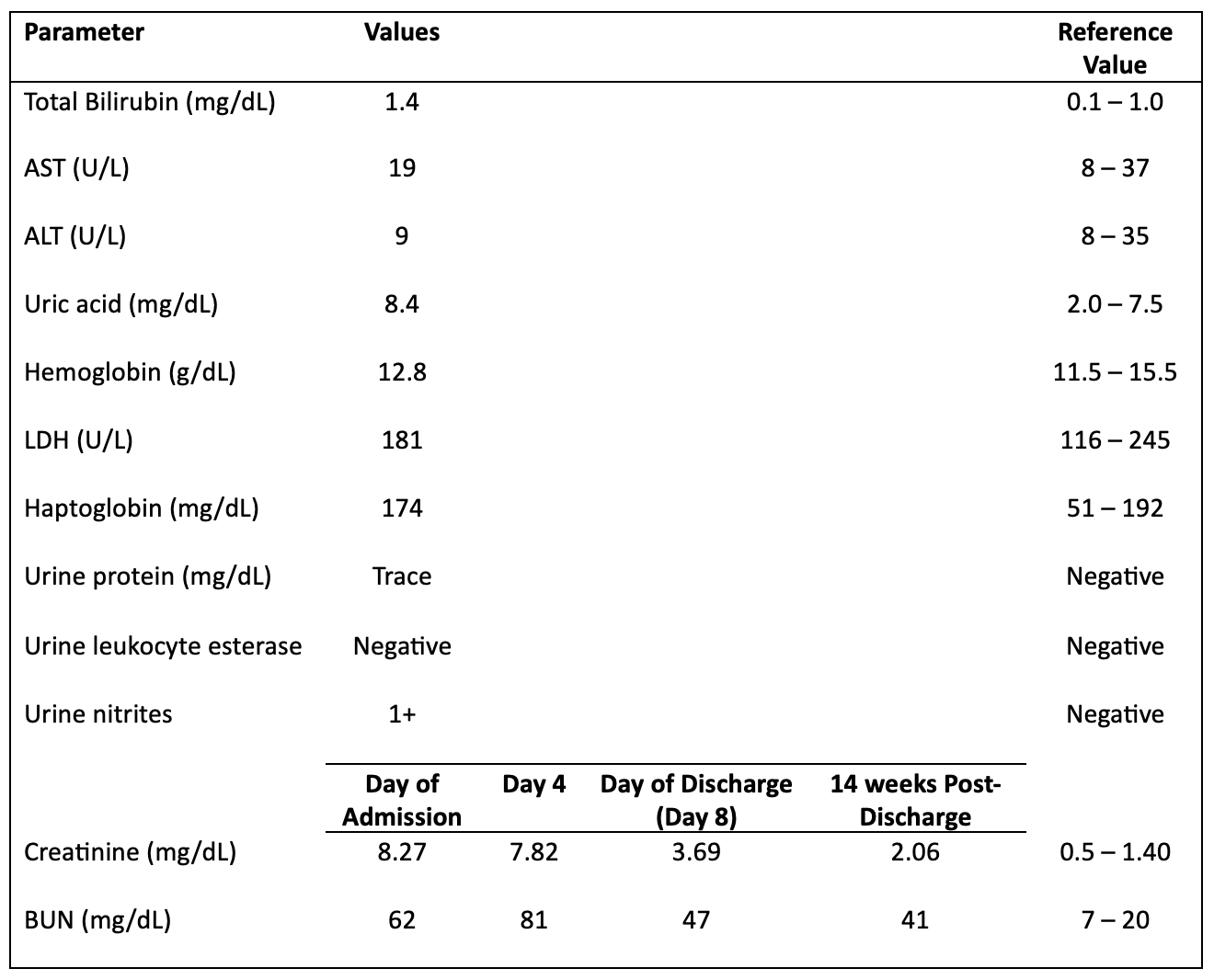
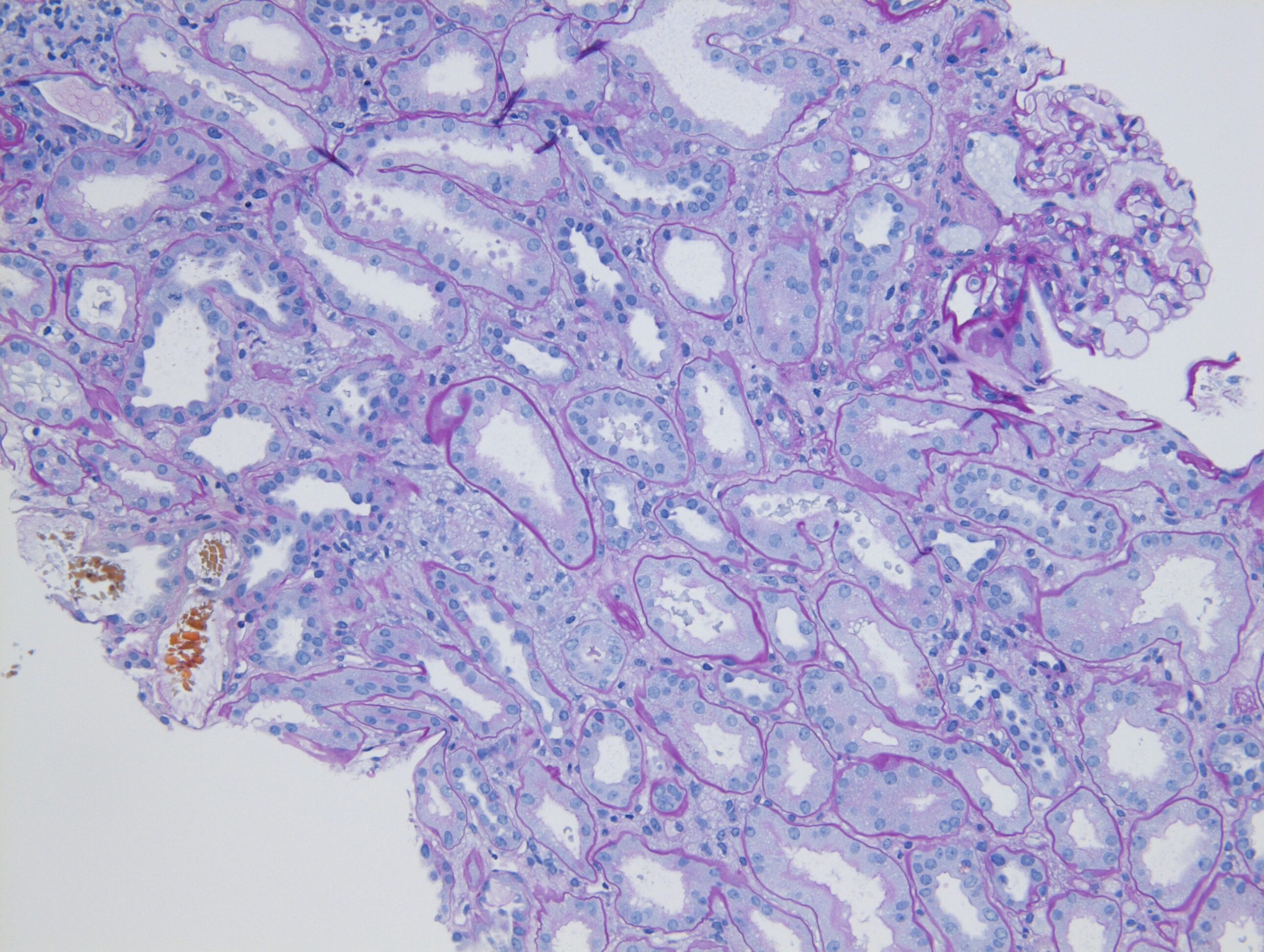
Case Presentation: A 66-year old woman, with a history of renal transplant for diabetes related end-stage renal disease, was admitted to the hospital by her transplant team, for significantly abnormal serum creatinine level of 8.6 mg/dL from her baseline creatinine value of 1.6 mg/dL. Of note, she underwent cystoscopy by urology 2 weeks prior for follow-up of her interstitial cystitis, and was prescribed a 10-day course of phenazopyridine 200 mg three times daily for post-procedural dysuria. Physical exam on presentation was notable only for right iliac fossa transplant-site tenderness. The pertinent laboratory markers are shown in Table 1. Her microscopic urinalysis demonstrated rhomboid crystals on urinary sediments. Transplant renal ultrasound did not show evidence of transplant hydronephrosis, nephrolithiasis, or any other pathology. Nephrology team was consulted, who recommended biopsy of the transplanted kidney. The pathology revealed acute tubular injury with a presence of yellow crystalline material, which was neither consistent with urate nephropathy, nor with oxalosis or 2,8-dihydroxyadeninuria. (Figure 1) Given the temporal association of phenazopyridine with the patient’s acute kidney injury, it was concluded that the presentation suggested crystalline nephropathy associated with the medication. Intravenous sodium bicarbonate drip was administered to alkalinize urine for over 48 hours. With withdrawal of the nephrotoxic agents and administration of intravenous fluids, her kidney function slowly began to improve and she was discharged with close outpatient nephrology follow up, where she continues to show a sustained recovery with the most recent creatinine value of 2.06 mg/dL.
Discussion: Phenazopyridine is a commonly used urinary analgesic in the outpatient setting to relieve lower urinary tract symptoms in urinary tract infections or in surgical patients in perioperative period. Though the medication is readily available, it has been associated with development of acute renal failure at supratherapeutic doses, especially in those with preexisting chronic kidney disease (CKD). Nephrotoxicity associated with it has been described as acute interstitial nephritis or renal tubular necrosis, and it is usually accompanied by hemolytic anemia, yellow discoloration of skin and methemoglobinemia.Here we describe a unique case of isolated acute kidney injury (no evidence of hemolysis or other pathology), secondary to yellow crystalline nephropathy from phenazopyridine use in a renal transplant patient with CKD, resulting in severe acute kidney injury. From our review of literature, such crystalline tubular deposition in association with the drug has not been reported. Exact mechanism related to the drug’s nephrotoxicity is unclear, but it appears to be dose dependent and associated with diminished renal excretion. Thus, providers should be vigilant in prescribing this medication in those with a history of CKD; and should try to avoid it in renal transplant recipients unless under a transplant nephrologist’s supervision.
Conclusions: Though the general recommendations suggest to avoid use of phenazopyridine in those with glomerular filtration rate (GFR)< 50 ml/min/1.73m2, we advise utmost caution with its use in patients with any degree of renal impairment, and recommend avoiding it in renal transplant patients unless absolutely warranted and only under supervision of a transplant nephrology team.