Background: To date, attempts at estimating diagnostic error (DE), as defined as missed, incorrect, or delayed diagnoses, have focused on the identification of all types of adverse events, not specifically DE. Retrospectively identifying and ascertaining DE for hospitalized patients has been further challenged by (1) variability in operational definitions of DE; (2) use of non-standardized and low sensitivity data collection instruments; and (3) low positive predictive value (PPV) of measuring DE in a random sample of patients. Recent studies have suggested that specific types of clinical events in the EHR or “e-triggers” may enrich a cohort with cases likely to have DE, thereby increasing the PPV of DE for that trigger-positive cohort. The purpose of this analysis is to estimate the prevalence of DE in the hospital setting. We achieve this by using a standardized validated chart review tool to ascertain DE in a stratified cohort of cases randomly selected by specific e-trigger events with variable hypothesized likelihoods of DE.
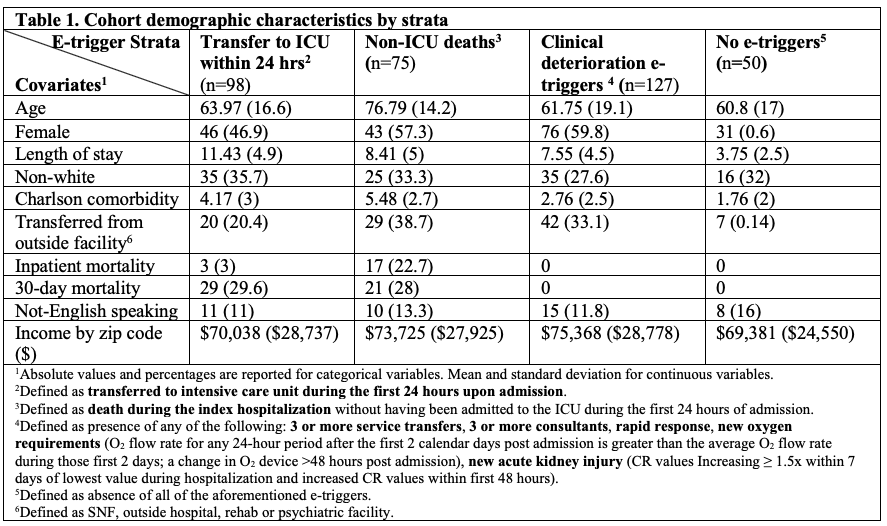
Methods: Our population was defined as patients who were hospitalized on the general medicine service at a large academic medical center in Boston, MA from July 2019 to March 2020. We used stratified random sampling to assemble a cohort of patients based on a priori selected e-triggers (Table 1) with high likelihood of DE (e.g., ICU transfer, death, clinical deterioration markers), restricting length of stay (LOS) of 21 days or less. Diagnostic error was ascertained independently by two clinician reviewers who conducted structured chart reviews using validated instruments (SaferDx instrument, DEER taxonomy) which we previously adapted for acute care. All cases were adjudicated by reviewers until consensus was reached. Cases in which consensus was not attained were sent for tertiary review by an expert review panel to resolve all discrepancies. We calculated the prevalence of DE for each stratum from which we calculated the unbiased prevalence estimate for the entire population and corresponding 95% confidence intervals.
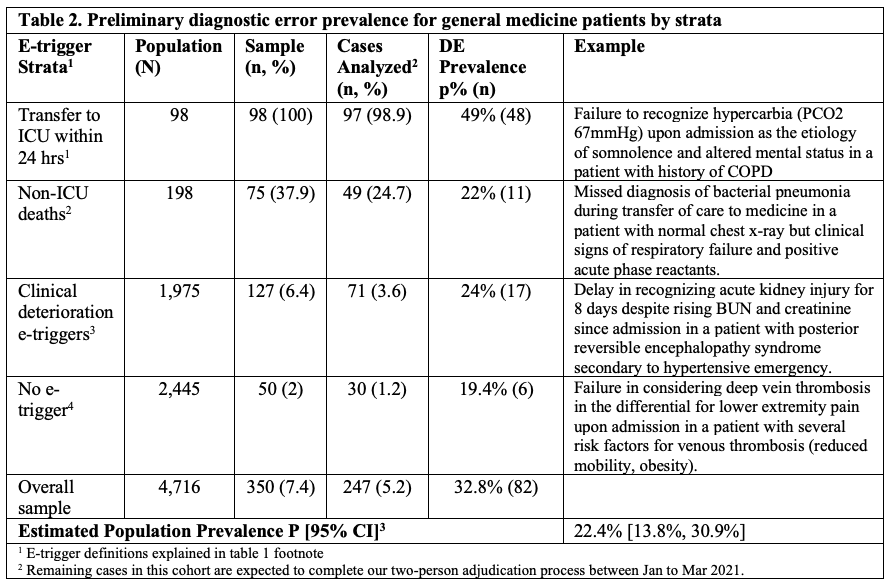
Results: A total of 4,716 patients (Table 1) were hospitalized between July 2019 to March 2020 with a LOS of 21 days or less and had the following distribution of e-trigger events: 98 (2%) transferred to ICU within 24 hours of admission; 198 (4.2%) died during hospitalization (but not transferred to the ICU); 1,975 (36%) had at least one clinical deterioration marker (defined in Table 1); and 2,445 (51.8%) had none of the aforementioned e-triggers. A random stratified cohort of 350 patients was created using the following proportions of e-trigger events: ICU transfers (100%), non-ICU deaths (38%), clinical deterioration triggers (6.4%), no triggers (2%). To date, 247 cases have been reviewed, adjudicated, and analyzed. Diagnostic error prevalence per strata, corresponding examples, and the estimated prevalence for the overall population are shown in Table 2.
Conclusions: At a large academic medical center, the prevalence of DE among patients with lengths of stay of 21 days or less was 22%.