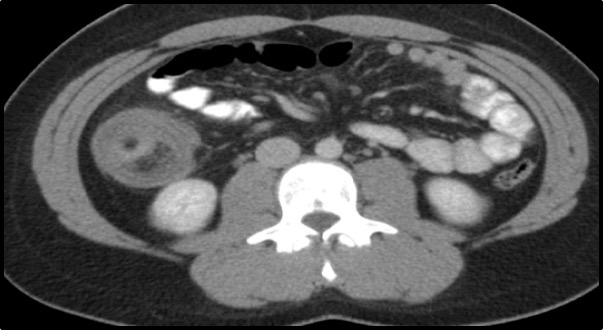
Case Presentation: A 22-year-old female with a past medical history of cholecystectomy and bipolar disorder presented with left upper quadrant spastic abdominal pain 9/10 in intensity, radiating to the epigastrium for the last 5 days, along with intermittent nausea, vomiting, and diarrhea. The patient described her bowel movements as a green ribbon-like consistency with no stains of blood. On admission her vitals were stable, physical examination was remarkable for diffuse abdominal tenderness, most notable in the left upper quadrant. CT scan of the abdomen revealed an ileocolic intussusception with small bowel obstruction. A 2.9 cm rounded fat attenuation structure is seen within the lumen of the ascending colon in this region, suspicious for intraluminal lipoma as the lead point. The patient had laparoscopic right hemicolectomy. Intraoperatively a firm intussusception at the ileocecal junction involving the terminal ileum was seen. It was not manually reducible.There was also an obstructive appearance with a dilated proximal small bowel. Pathology of the specimens from the right colon, terminal ileum surprisingly showed findings consistent with submucosal leiomyoma not a lipoma.
Discussion: Intussusception refers to the process wherein a segment of the intestine telescopes into a more distal segment. Relatively common in children, it is a rare occurrence in adults. In most clinical scenarios patients present with abdominal pain, intermittent partial bowel obstruction that is associated with fever, weight loss, constipation, nausea, vomiting. Diagnoses is established with an abdominal CT scan that shows the classical target/doughnut sign and sausage-shaped mass (4,5). Most cases of intussusception in adults require surgical resection rather than reduction (5). In terms of the management of leiomyomas causing intussusception with obstruction, the treatment is surgical removal (5). Malignancy is often the inciting cause of intussusception in adults. The findings of leiomyoma in this case of intussusception in a young female makes this case very unique. The findings, in this case, displays that there is still much mystery to the causes of abdominal pain in adults, more so in this case of intussusception.
Conclusions: Adult Intussusception is a rarity with an occurrence of less than 5% in adulthood (1). Most common causes in adults are due to a pathologic lead point within the bowel, with malignancies occurring in greater than 50% of cases (1). On the occasion this pathology does occur, it causes an obstruction in about 1-5% of patients (1,2). Normally about 80-90% of these events are seen in children younger than two years of age with a 3:2 male predominance (3). Given the extremely low rate of mechanical bowel obstruction occurring due to intussusception, coupled with its clinical nonspecific presentation, there are many unique challenges to the diagnostic and management approach. However it is still recommended that an abdominal CT scan be done to aid in the diagnosis. Adult cases of intussusception is mainly manage with surgical resection.