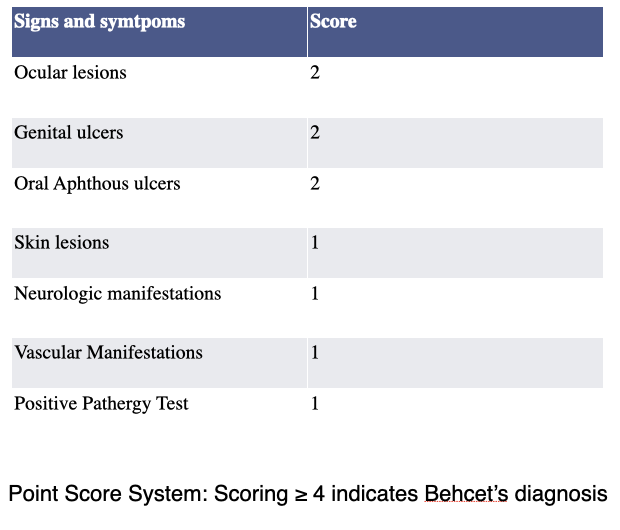
Case Presentation: A 41 years-old Scottish male patient with a past medical history significant for erectile dysfunction, prior EBV infection, hyperlipidemia, umbilical hernia, and urethral meatal stenosis was referred by his PCP to rheumatology for oral thrush and recurrent oral ulcers for 3 years. The patient was initially seen by an Infectious disease doctor who reported resolution of oral thrush with clotrimazole troches. However oral ulcers remained unresolved with nystatin, and magic mouthwash, and was seen by an oral surgeon for a biopsy which was non-diagnostic and negative for HSV. He later developed burning micturition and a purple hue at the urethral meatus with a genital/scrotal ulcer. The patient was presumed to have UTI and treated with ciprofloxacin, which resolved dysuria but not genital lesions. The patient was then referred to a rheumatology clinic for further evaluation to rule out autoimmune etiology. ANA, Anti ds DNA, ASCA, MPO, PR3, Coombs test, CMV, Hepatitis panel, and STI testing- HIV, Chlamydia PCR, and RPR were sent for analysis which reported negative, however, he was found to have positive HLA B51 and was diagnosed with Behçet’s disease. Per the International criteria for Behçet’s disease scoring system, patient having ≥4 points have been classified as having Behçet’s disease. He was treated with topical steroids as needed, and colchicine was used to prevent recurrence, which showed a remarkable response.
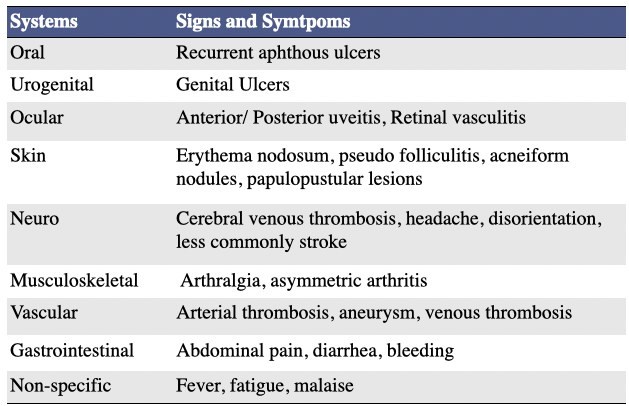
Discussion: Oral ulcers are one of the most common complaints seen by general practitioners in their office. Recurrent aphthous stomatitis affects roughly 20% of the general population, incidence varies from 5-50% depending on the ethnic and socioeconomic groups investigated. Oral ulcers could be one of the common presentations of a rare autoimmune systemic vasculitis syndrome – Behçet’s disease, which often manifests as a cluster of symptoms that may include uveitis, mucocutaneous ulcers in oral and/or genital areas. Per the International criteria for Behçet’s disease scoring system, patient having ≥4 points have been classified as having Behçet’s disease. Our patient had recurrent oral ulcers and genital ulcers accounting to 4 points- has been diagnosed with Behçet’s disease per The International Criteria for Behçet’s Disease Scoring System.The oral ulcers refractory to usual management like vitamin supplementation, anti-viral and symptomatic care, or recurrent in onset must be investigated further. Including Behçet’s disease in the differential diagnoses of refractory oral ulcers is the key to avoiding the delay of care in these patients.
Conclusions: It is often a common practice to treat mucositis/oral ulcers or genital ulcers with symptomatic care, however, general practitioners should keep reasonable alertness of possible Behçet’s disease when encountering a patient with recurrent mucositis and/or genital ulcers, which are refractory to the routine treatments. Early diagnosis and treatment of Behcet’s disease is vital to avoid poor outcomes, such as blindness and thrombosis.