Background: Burnout among hospital medicine providers is well known. Advanced practice providers (APPs) are well-established in hospital medicine but there is a lack of data on burnout specific to the physician-APP model. As more hospitalist groups staff a physician-APP model, identifying contributors to burnout is key for ensuring career sustainability. Our academic hospital medicine group at a tertiary medical center has a service staffed by both physicians and nurse practitioners.
Purpose: Burnout and contributing factors were measured using a survey distributed to nurse practitioners and physicians. Specific interventions designed to impact key negative factors in both providers were implemented.
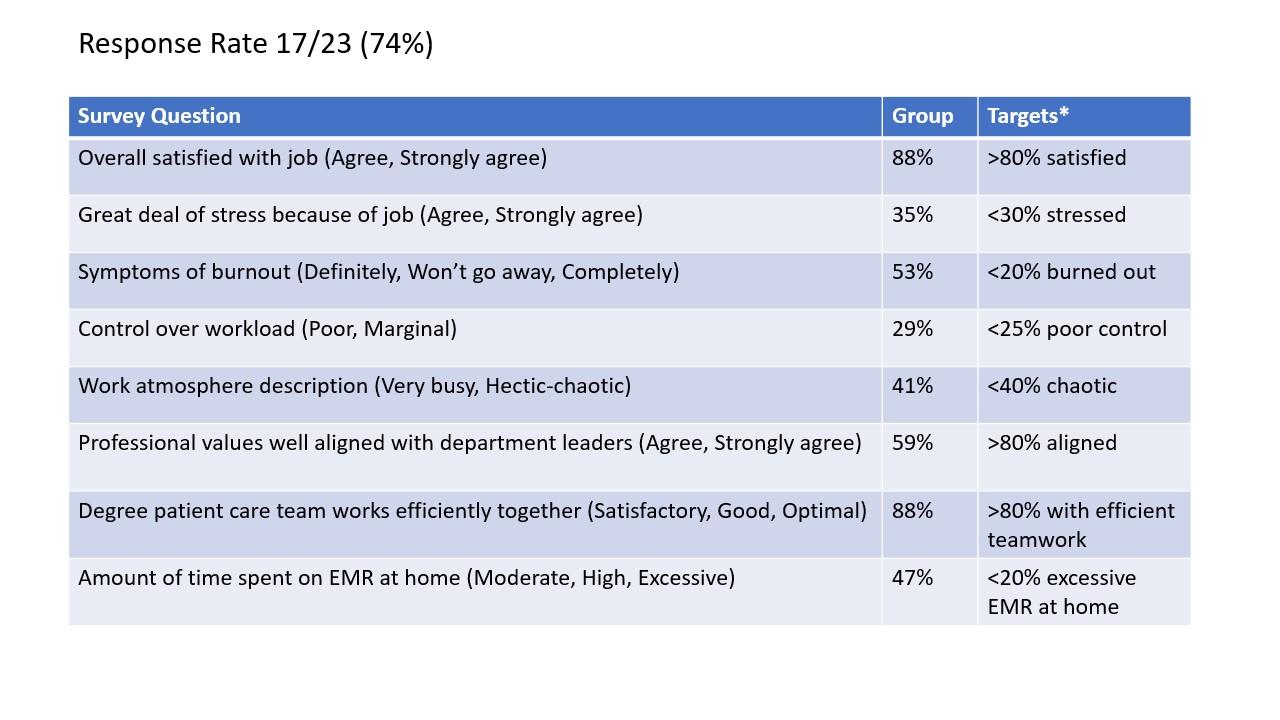
Description: Using the Mini Z assessment tool and an anonymous online survey platform we measured burnout in our group. We identified a high level of burnout, 53%, among all providers in our group. The highest rate of burnout (67%) was found in those who rotated on the NP/MD service greater than 4 weeks per year. The most prevalent sources of discontent were the 12-hour day shift, responding to calls from outside hospitals for patient transfers, and variability in team rounding structure. As a result of this assessment, we reduced the total number of in-hospital hours required of the physician by 1.5 hours. The NPs provided independent in-hospital coverage with phone access to physicians. To address the burden of calls for outside transfers, we arranged for 3 hours of telephone coverage to allow the physicians and NPs to collaborate on patient care. The calls were covered by other physicians on a rotating basis to evenly distribute calls.
To improve efficiency and provider satisfaction, we defined the division of clinical and administrative work between the physicians and NPs and outlined a structure for providers to round. This allowed the NPs to have more autonomous time to make treatment decisions. It emphasized a collaborative approach to all work required on the service where the physicians shared administrative tasks that were traditionally completed by the nurse practitioners.
Conclusions: Our interventions of a small reduction in shift hours for physicians, sharing calls for outside hospital transfers, and creating expectations for work on the NP/MD service with increased APP autonomy addressed the identified causes of burnout in all providers. These changes were designed to decrease burnout for both physicians and APPs in parallel. Our intervention is the first to address Hospitalist APP burnout by increasing clinical autonomy.
1. Roberts DL, Shanafelt TD, Dyrbye LN, West CP. A national comparison of burnout and work-life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014 Mar;9(3):176-81.