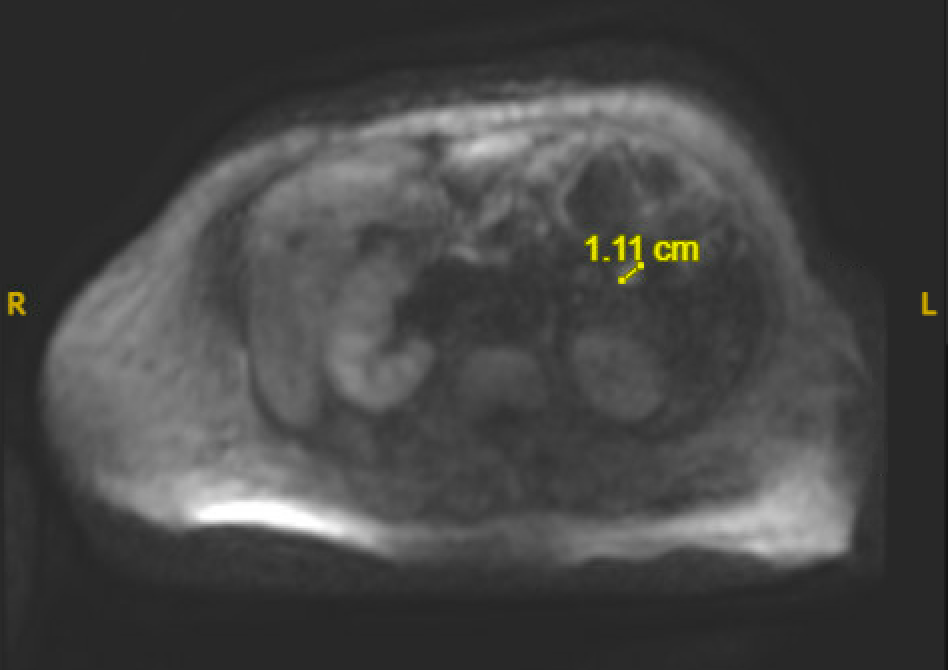
Case Presentation: A 63-year-old female with a history of heart failure with reduced ejection fraction and pre-diabetes presented to the hospital with lower extremity weakness. On presentation, her physical exam was significant for bilateral lower extremity pitting edema and hepatomegaly. Lab work showed an elevated total bilirubin (7.3mg/dL) and direct bilirubin (3.8mg/dL), liver function tests (AST 675, ALT 493), and brain natriuretic peptide (1397.3pg/mL). She was admitted for treatment of heart failure exacerbation as well as for workup of her acute liver injury. During her hospital admission, she had several episodes of symptomatic hypoglycemia characterized by feeling weak and tremulous with venous glucose < 40mg/dL. Her symptoms improved with dextrose infusions. Further work up revealed an elevated C-peptide (8.6ng/mL), inappropriately normal insulin level (3.4μU/mL), proinsulin (6.8pmol/L), low insulin-like growth factor-2, negative insulin antibody, A1c of 5.7%. A CT of her abdomen/pelvis and later an MRI with Eovist contrast revealed a 1.1cm lesion in the proximal jejunum concerning for an insulin-secreting neuroendocrine tumor or gastroenterological stromal tumor. Other causes of hypoglycemia were ruled out as her symptoms persisted despite adequate nutrition, treatment of her heart failure, and improvement in her liver function to AST 55, ALT 31, total bilirubin 3.8mg/dL. Her blood alcohol level and cortisol were normal, and all drugs and medications side effects were ruled out including a negative sulfonylurea screen. The patient was treated with Octreotide, dextrose gel, and Glucerna shakes with improvement in her symptoms and venous glucose. On discharge, she had achieved normoglycemia but was given close follow up with Endocrinology and scheduled for a PET scan for further evaluation for metastatic disease.
Discussion: This case illustrates the uncommon finding of an insulin producing tumor. The incidence of insulinomas is estimated to be 1 to 4 per million person-years. Insulinomas are a rare cause of spontaneous hypoglycemia. In cases of spontaneous hypoglycemia, Whipple’s triad should be used to confirm hypoglycemia before initiating further workup. Whipple’s triad is characterized by three criteria: symptoms of hypoglycemia, a low plasma glucose, and resolution of symptoms after the plasma glucose is raised. After recognition of the triad, the next step is to rule out other causes of hypoglycemia including sepsis, heart and hepatic failure, medication side effect, alcohol induced, and poor nutrition. The role of insulin should be assessed next. As in this case, an elevated C-peptide, elevated proinsulin, and inappropriately normal insulin level suggested the presence of an insulinoma. Finally, imaging plays a significant role in confirming the finding of an insulinoma instead of a diffuse process. Treatment can be managed conservatively with medications such as Diazoxide or Octreotide, which both act to inhibit insulin release while awaiting definitive treatment with surgical removal.
Conclusions: Hypoglycemia has a wide differential and requires a thorough workup in non-diabetic patients. Insulinomas, while rare, can be easily diagnosed by biochemical testing confirming inappropriate hyperinsulinemia (end of fast insulin level of ≥3 μU/mL and a proinsulin level of ≥5 pmol/L). In every case of spontaneous, recurrent, or refractory hypoglycemia, insulinomas should be included in the differential diagnosis as they can be treated with surgery or with medications.