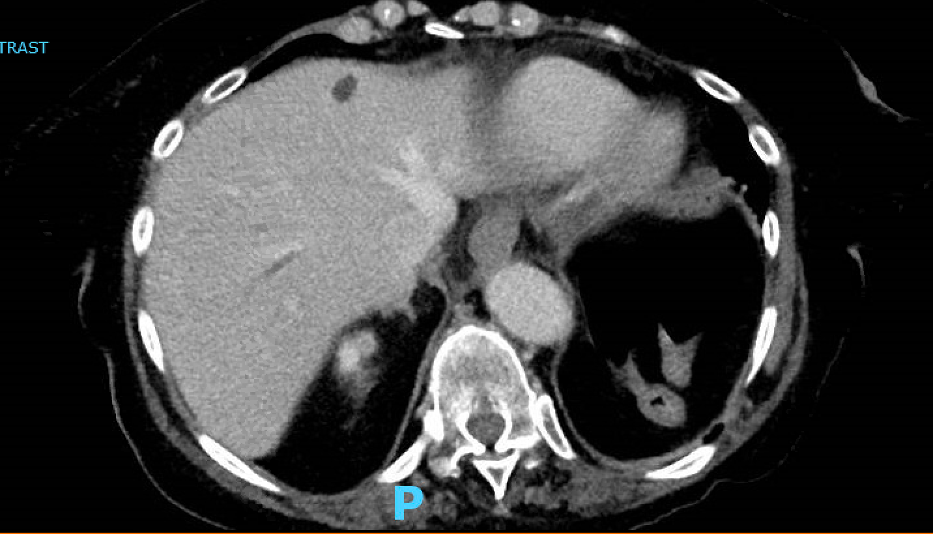
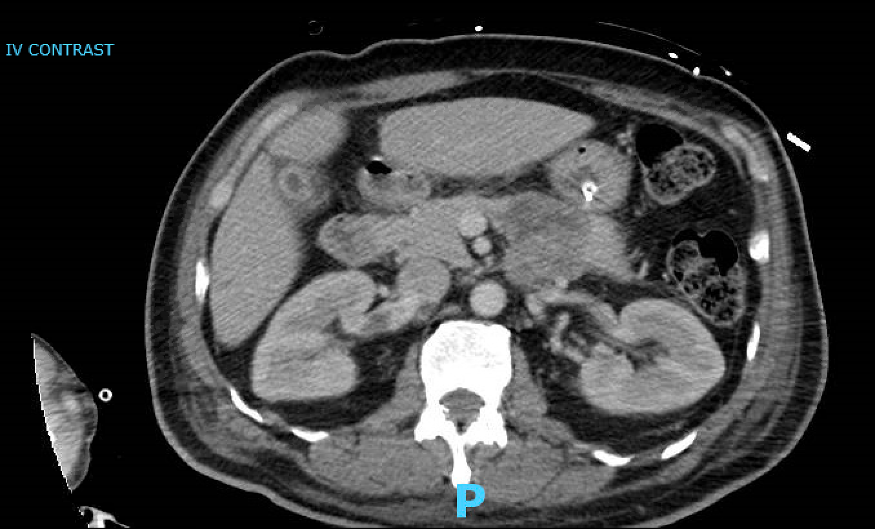
Case Presentation: Our first patient is a 75-year-old female with a history of hypertension, type 2 diabetes, hypothyroidism, rheumatoid arthritis, chronic kidney disease stage III, FSGS, and fibromyalgia who presented with a one-week history of midsternal chest pain, dyspnea on exertion, decreased exercise tolerance and epigastric discomfort. Vital signs were notable for tachypnea (22 bpm) and tachycardia (111 bpm). On physical exam, she was dyspneic when speaking with coarse breath sounds, trace bilateral lower extremity edema, and required 2L nasal cannula. Labs were significant for an INR 1.5, Troponin T 80ng/L, pCO2 59mmHg, RVP negative. On imaging, she was found to have bilateral pulmonary emboli and hepatic vein thrombosis (HVT) [Fig 1]. Workup also revealed a pancreatic mass which was biopsy proven benign. Patient was discharged on Eliquis for anticoagulation. Later she developed weakness and was diagnosed with Amyotrophic Lateral Sclerosis (ALS). Our second patient is a 62-year-old male with type 2 diabetes and hypertension who presented to the hospital for acute hypoxemic respiratory failure (AHRF) due to pneumonia and diabetic ketoacidosis. His hospital course was complicated by methicillin-resistant staphylococcus aureus infection and possible osteomyelitis of the spine causing discitis, anemia, and renal vein thrombosis (RVT) [Fig 2]. COVID-19 PCR was negative. Discharge was complicated by profound 45-pound weight loss, loss of appetite, and continued AHRF. He was eventually diagnosed with ALS and is now at home on AVAPS and hospice. His RVT resolved post-hospitalization and anticoagulation therapy.
Discussion: ALS is a progressive neurodegenerative disorder causing muscle weakness, and substantial disability in patients, and eventually death, with a mean survival of 3-5 years [1]. Its progression is associated with various life-threatening conditions, among them venous thromboembolisms (VTE). One prospective study showed a 1-year VTE incidence rate of 11.2%, and that subjects with leg-onset ALS or significant leg weakness had a 1-year VTE incidence rate of 35.8% and 35.5%, respectively [2]. Another study showed a rate of VTE of 8.5/100 patients-year in patients with ALS [3].The most probable mechanism for the increased incidence of VTE’s in ALS is from patient immobility secondary to muscle weakness. However, this mechanism is less convincing for RVT’s and HVT’s. When specifically looking at the incidence of these two pathologies in ALS patients, literature review yielded zero PubMed results. A possible explanation could be hypercoagulability from a pro-inflammatory state in ALS. MS analysis of blood in ALS patients has shown to be downregulated coagulation pathways with upregulation of the complement pathway, which could potentially trigger the clotting cascade [4]. Another study showed that neurodegeneration in ALS can lead to clotting cascade activation and that signaling molecules involved in coagulation processes such as thrombin, thrombomodulin, HMGB1, and DAMPs can play a role in neural damage [5]. Thus, measurement of these molecules in serum could serve as a potential screening tool for identifying ALS patients at risk for coagulopathy.
Conclusions: We believe that these are the first cases linking ALS and RVT or HVT in the literature. For both patients, the ALS diagnosis was preceded by RVT or HVT. Therefore, we recommend that when a patient is diagnosed with RVT or HVT and all other causes are ruled out, consider evaluating for ALS.