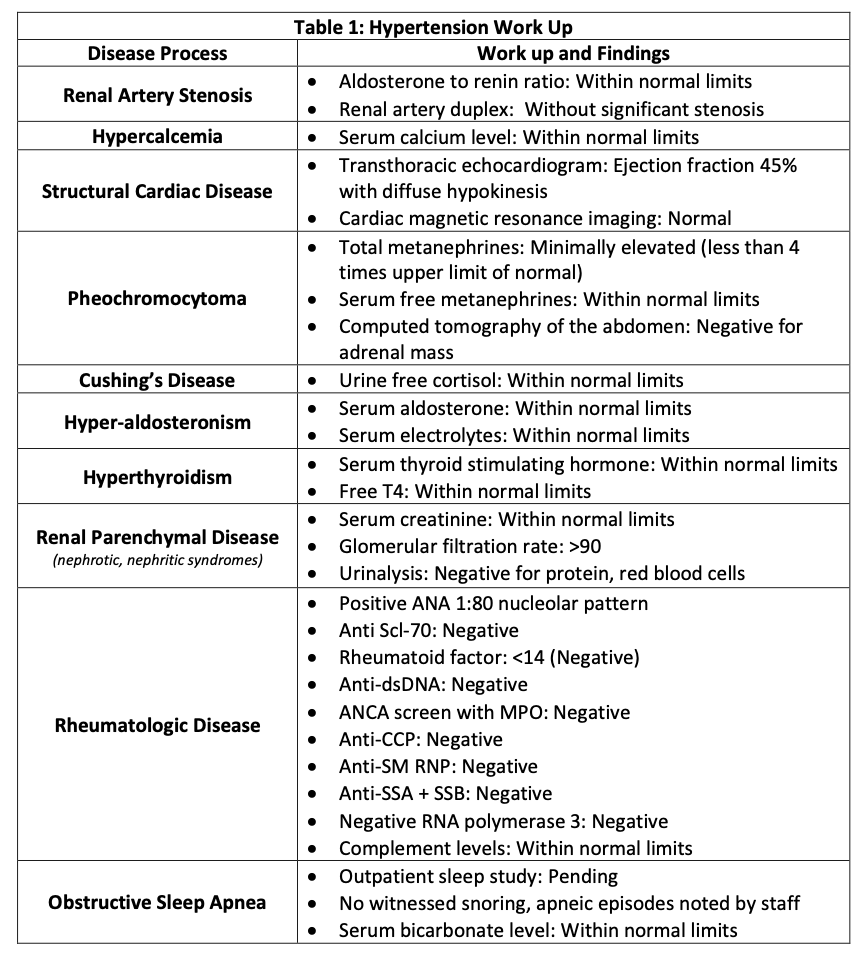
Case Presentation: Patient is a 45-year-old female with a history of esophageal reflux and dysmotility, asthma, depression/anxiety, and recent SARS-2-CoV infection (COVID-19) who presented to our hospital 9 months after initial and 3 months after recurrent COVID-19 with headache, dyspnea, and home blood pressures (BP) > 180/100. Patient reported intermittent symptoms for the last 3 months requiring multiple hospitalizations for intravenous (IV) anti-hypertensive medications (anti-HTNs). Review of systems was notable for palpitations, flushing, and daily diarrhea. Documentation from outside hospitals noted robust response to IV medications, but the patient was unable to manage her BP in the outpatient setting despite adherence to her home regimen of carvedilol 25 milligrams (mg) twice daily (BID), losartan 100 mg daily, furosemide 20 mg daily, clonidine 0.1 mg BID, and nifedipine 60 mg BID. She was found to have BP of 215/144 and pulmonary edema on chest radiograph. She received IV labetalol, IV furosemide, and nitroglycerin with improvement of BP to the 160s and was subsequently admitted for hypertensive emergency. A secondary hypertension (HTN) work-up was pursued but grossly unremarkable (Table 1). Other considered etiologies included dysautonomia and paraganglioma, both of which were deferred to the outpatient setting. However, the patient was unable to be safely discharged due to persistently elevated BP. Review of vital trends revealed episodes of hypotension after IV anti-HTNs and interestingly, the patient reported passing full medication tablets in her stool on multiple occasions. This prompted concern that route of administration may be a limiting factor in management. An inpatient colonoscopy with tissue biopsy was pursued but did not reveal structural or histological abnormality and celiac panel was negative. However, stool studies demonstrated a high fecal osmolar gap, supporting the presence of digestive abnormalities. Thereafter, clonidine was transitioned to a patch and the patient’s mean BP improved, indicating a potential inability to adequately digest oral anti-HTN pills. Ultimately, liquid formulations of previously trialed medications (labetalol, amlodipine, spironolactone) were administered with successful BP control.
Discussion: Here we present a case of resistant HTN in a patient with chronic diarrhea who ultimately responded to liquid-based formulations of anti-HTNs post COVID-19 infection. There has been an association between COVID-19, new-onset HTN (1) and chronic diarrhea (2-3). This may be due to ACE-2 mediated entry and viral damage of the vascular endothelial cells and intestinal brush border cells, respectively. Furthermore, ACE-2 expression on the intestinal brush border cells can cause inflammation leading to gut hypopermeability and subsequent osmotic diarrhea with increased osmolar gap. This may lead to decreased efficacy of pill formulated medications and require further investigation into malabsorptive processes secondary to COVID-19.
Conclusions: Patients with difficult to treat complications after COVID-19 infection require a broad systems-based approach. In our case, the efficacy of liquid-based formulation of the anti-HTNs over the traditional pill-based implicates a possible larger role of the damage to the intestinal brush border cells in the digestive system. Further investigations of the pathophysiology of post-COVID-19 HTN and malabsorption syndromes may help inform future treatment.