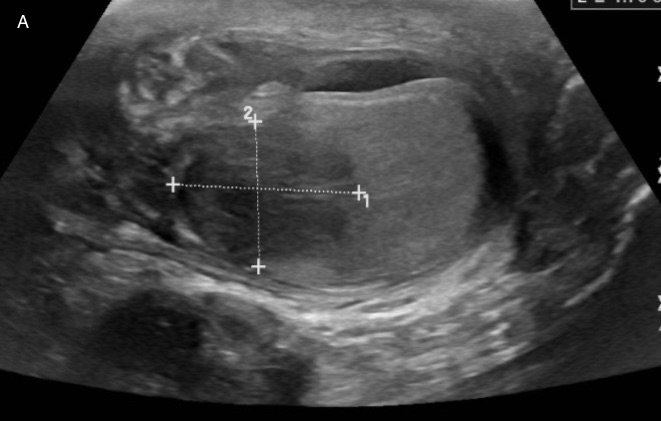
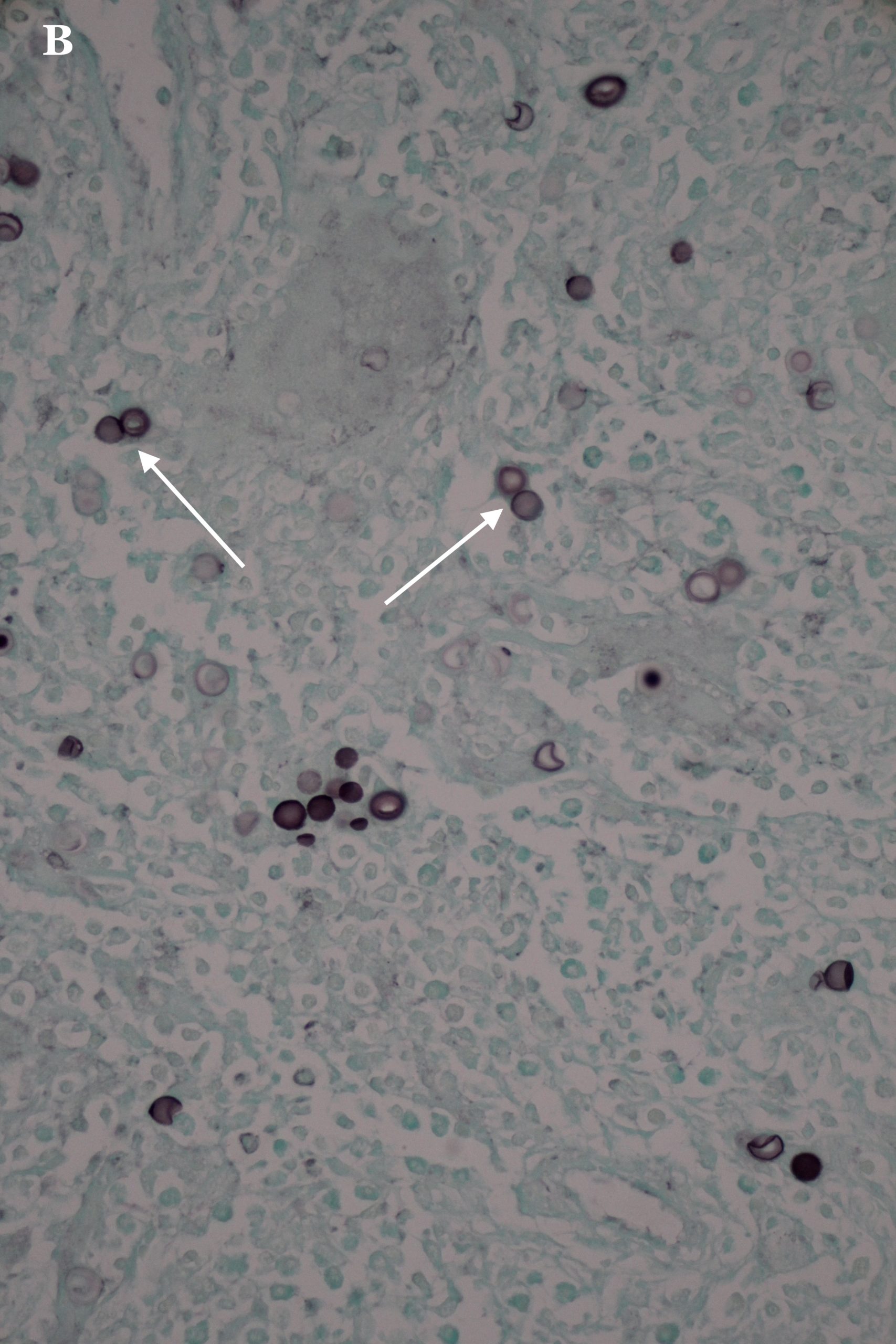
Case Presentation: A 44-year old Chin-Mizo speaking male with a history of stage IV non-small cell lung cancer presented to the Emergency Department with acute-onset hematuria and painless right testicular swelling. Physical examination revealed an enlarged right hemi-scrotal mass and painful nodular skin lesion on right posterior calf. A transverse ultrasound image of the scrotum showed mass-like hypoechoic lesion in the right testicle measuring approximately 2.3 x 1.8 cm (Panel A) and a corresponding color Doppler image showed an asymmetric hypervascularity of the right testicle and epididymis. A PET CT scan confirmed a lobulated and hypermetabolic mass in the right scrotum measuring 4.7 x 3.4 cm. MRI of right lower leg showed a cystic-like lesion in the periphery of the lateral gastrocnemius muscle. The patient underwent right inguinal orchiectomy along with biopsy of the leg lesion. Histopathology of right testis H&E stain revealed necrotizing acute and chronic diffuse granulomatous inflammation with giant cells surrounded by fungi. A GMS stain showed broad based budding yeast (arrows, Panel B). Tissue culture grew Blastomyces dermatitidis/gilchristii. Given these findings, the patient was diagnosed with disseminated Blastomycosis. Patient was started on treatment with Amphotericin B and transitioned to Itraconazole upon discharge with recommendation to follow with Infectious Disease in outpatient clinic.
Discussion: Blastomycosis is a systemic pyogranulomatous infection that can disseminate to involve any organ in the body and mimic other granulomatous infections such as tuberculosis. Most common involved extrapulmonary sites of infection include skin, bones, and genitourinary system with commonly affected sites are prostate and epididymis. The infection occurs with increased frequency in the Great Lakes, Southeast and along the Ohio and Mississippi river valleys. Other risk factors include immunosuppression and outdoor occupation. Blastomycosis is acquired by inhalation of the spores and disseminates from a primary pulmonary infection to other organs by lymphohematogenous spread. The patient’s bronchoscopic culture was negative for infection. Given the mass-like appearance on scrotal US, a malignancy vs epididymo-orchitis was initially considered. The increased flow within the testicular lesion and epididymis is suggestive of an inflammatory cause and the mass in the testicle was well defined as opposed to the typical ill-defined appearance of orchitis.
Conclusions: Although the sonographic appearance of genitourinary blastomycosis is non-specific, hospitalists need to keep a high index of suspicious in the appropriate clinical setting, especially in immunocompromised patients not improving with antibiotics.