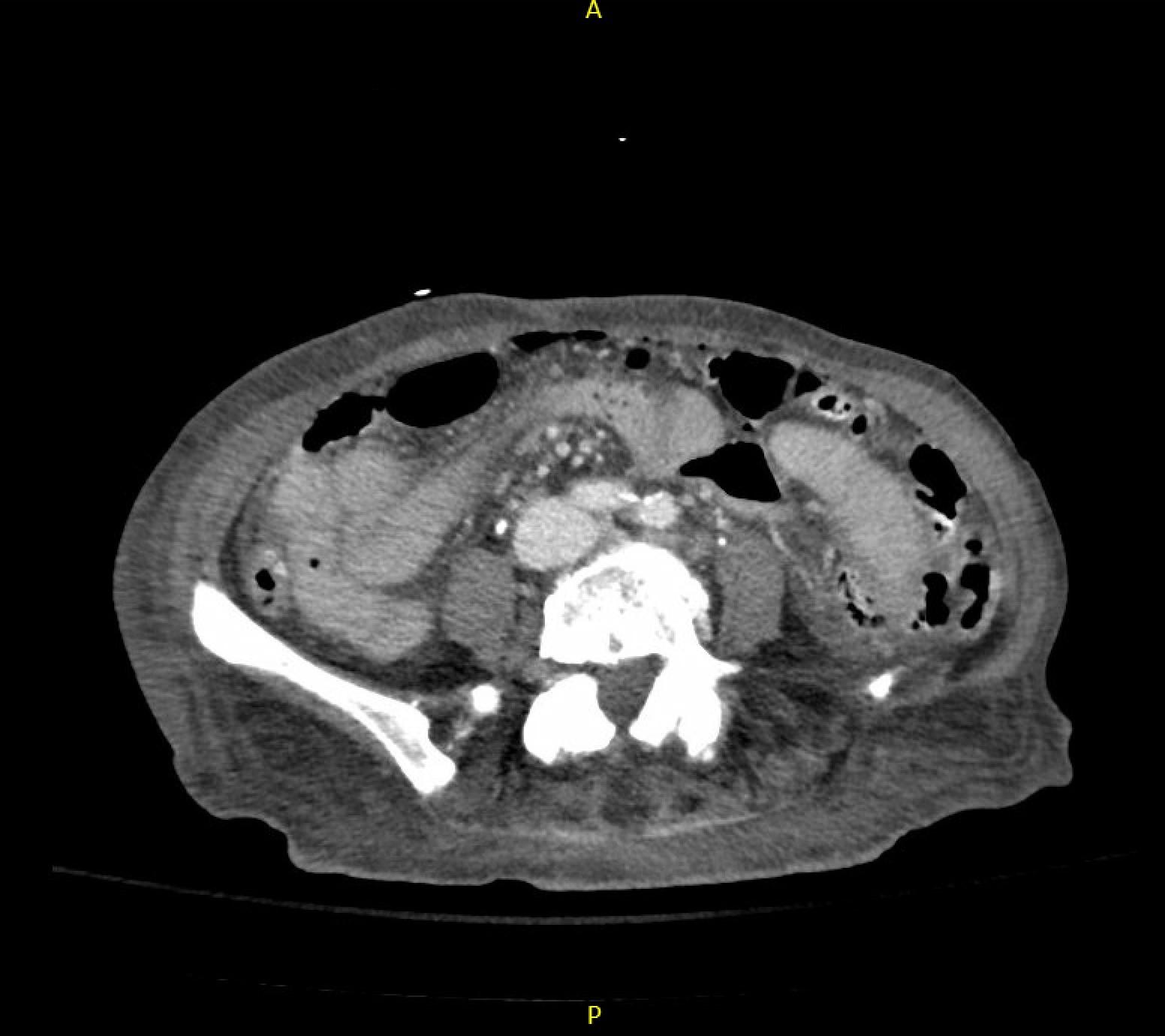
Case Presentation: An 80-year-old female with a past medical history of atrial fibrillation on daily aspirin, previously managed with Eliquis but discontinued due to multiple GI bleeds of unknown origin, and unexplained leukocytosis up to 61.67K, transferred to an academic hospital from a community hospital for two episodes of hematochezia and symptomatic anemia with a hemoglobin (Hgb) of 7.3 g/dL. She endorsed a 25 lb weight loss over four months. On exam the patient was alert and oriented with an irregular heart rhythm and tachycardia. Pertinent labs included a Hgb of 9 g/dL after 2 units of packed red blood cells, WBC 61.67K with ANC 42.37K, and aPTT 40. While admitted, patient continued to experience episodes of bloody diarrhea. Per recommendations from Gastroenterology a heparin drip was started to improve the sensitivity of a tagged RBC scan given prior negative results. While on heparin, the patient’s mental status deteriorated rapidly and she developed severe abdominal pain with signs of acute abdomen. CT abdomen pelvis revealed interval development of pneumoperitoneum and free fluid in the abdomen. Patient was emergently taken to the OR for an exploratory laparotomy. A small bowel perforation with an associated mass was resected with final pathology results revealing a diffuse large-B-cell lymphoma (DLBCL), with features of aggressive subtype (double-expressor, Ki67>95%). Given her poor prognosis, Palliative Care was consulted, and after extensive discussions with family, the patient was terminally extubated five days later.
Discussion: DLBCL is the most common lymphoid malignancy in adults1. Double-expressor lymphomas (DEL), which account for 20% to 30% of DLBCL cases and overexpress MYC and BCL2 proteins, are aggressive DLBCLs and associated with poor outcomes2. Although the GI tract is the most common extranodal site involved in non-Hodgkin lymphoma (NHL), primary gastrointestinal NHL is rare, accounting for 10-15% of NHL and 30-40% of extranodal NHL4. The most frequent sites of occurrence in primary GI NHL is the stomach, followed by the small intestine and ileocecal region3. GI obstruction is the most common complication, followed by hemorrhage and perforation4. In addition, the most frequent complaint is abdominal pain, followed by bloody feces and diarrhea4. We describe an atypical case of a small bowel perforation from an aggressive phenotype of DLBCL that initially presented as a GI bleed in the setting of unintentional weight loss.
Conclusions: DLBCLs, while aggressive, are potentially curable malignancies with the International Prognostic Index (IPI) and age adjusted IPI (aaIPI) being standards of prognosis1. MYC/BCL2 DEL is an aggressive B cell lymphoma and in elderly patients (>60 years, aaIPI=0-3) present a poor prognosis. In this case, our patient’s clinical presentation along with laboratory and imaging findings warranted examination for underlying hematologic malignancy, especially in the setting of neutrophilic leukocytosis and weight loss. While fit elderly patients with minimal comorbidities typically tolerate treatment to remission, given our patient’s age and her degree of debility and frailty status post exploratory laparotomy and small bowel resection with splenectomy, lymphoma-related treatment interventions were impractical. This case underscores the importance of promptly addressing acute issues in patients presenting with abdominal pain and hematochezia, while also investigating less emergent secondary etiologies, pending clinical stability.