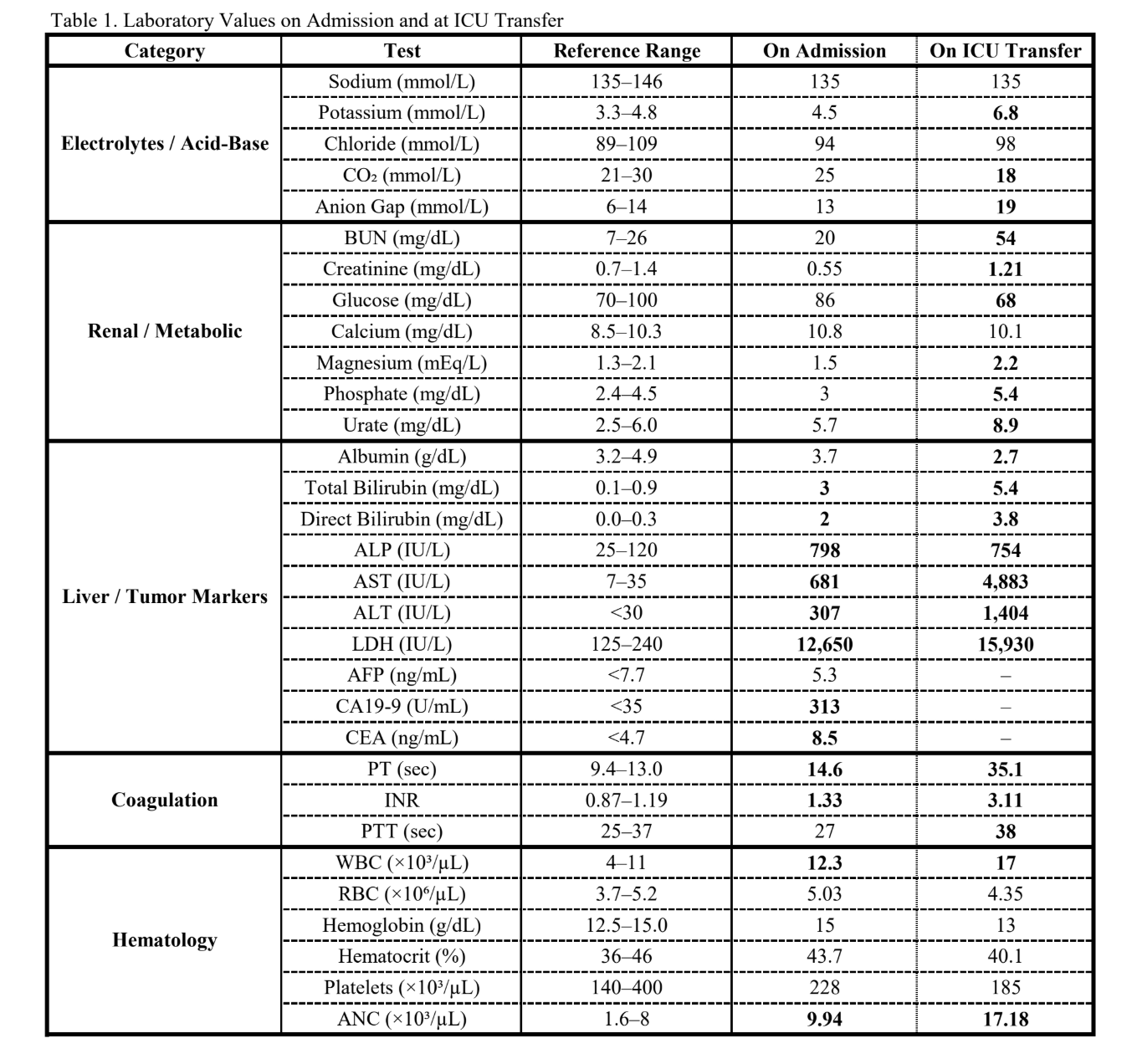
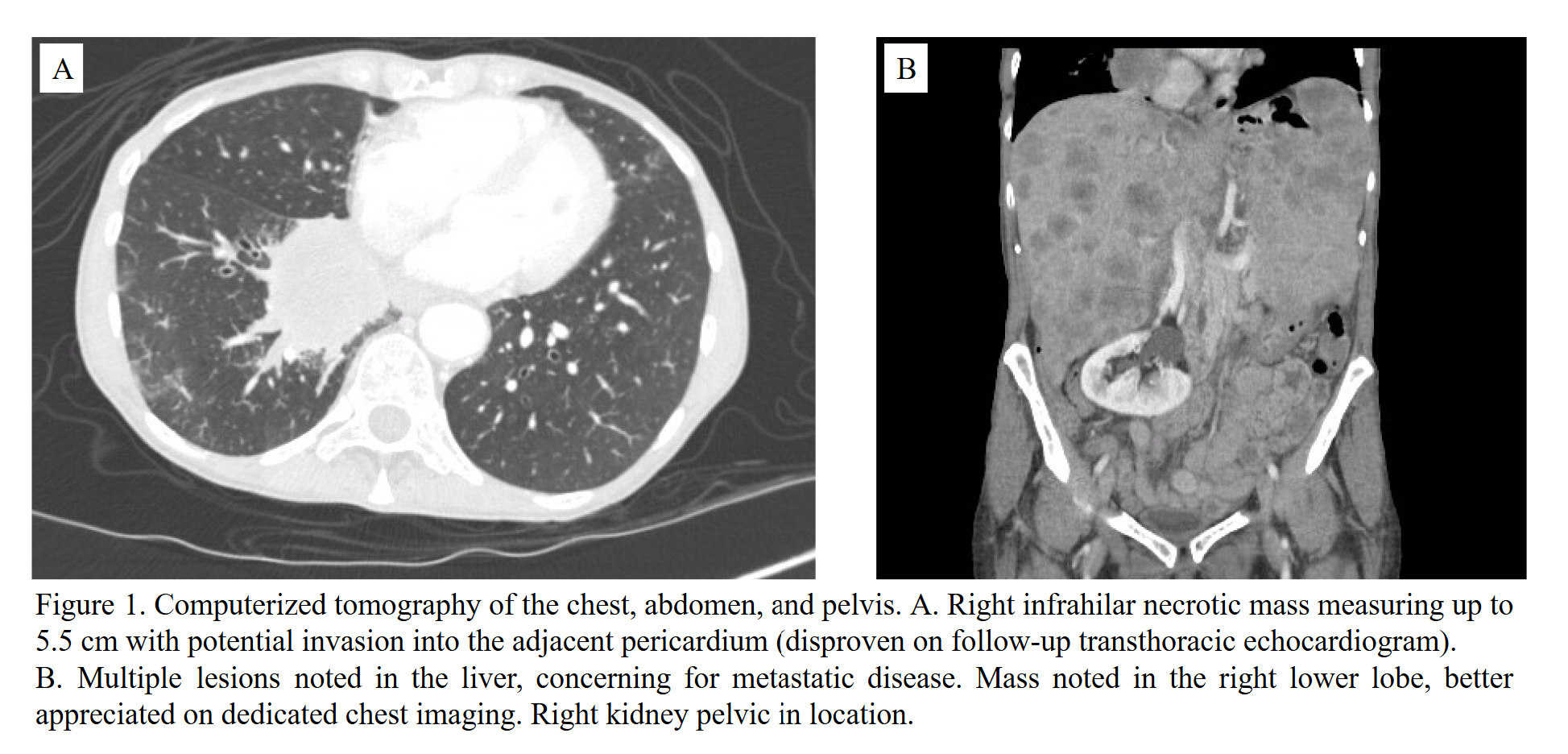
Case Presentation: Tumor lysis syndrome (TLS) is a life-threatening oncologic emergency characterized by acute metabolic derangements and potential end-organ damage following rapid cell breakdown. It typically arises after chemotherapy-induced tumor cell lysis, and is most often associated with malignancies featuring high cell turnover and tumor burden [1]. While TLS is well described in these settings, it can also occur spontaneously and, though rare, has been reported in solid tumors [2]. Systematic reviews and case reports have identified a handful of sTLS occurrences in lung cancer, with very few specifically involving squamous cell histology, reflecting the scarcity of data on this process and its outcomes [2-5]. We present a fatal case of sTLS in a patient with previously undiagnosed, widely metastatic, poorly differentiated squamous cell carcinoma of the lung.A 68-year-old woman with past medical history of ductal carcinoma in situ treated in 2006 presented to an outside ED with constipation, fecal incontinence, and progressive fatigue. CT imaging of the abdomen and pelvis revealed a large right lower lobe lung mass with multiple hepatic lesions concerning for metastatic malignancy. She initially declined inpatient evaluation but subsequently agreed to admission the following day after outpatient oncology consultation. Dedicated CT chest imaging demonstrated a 5.5-cm necrotic right infra-hilar mass with suspected pericardial invasion, pleural nodules, osseous metastases, and tumor thrombus in a pulmonary vein branch. A liver lesion biopsy was performed for diagnosis early in her hospitalization. Several days into hospitalization, she developed acute liver dysfunction, worsening creatinine, hyperkalemia, hyperphosphatemia, elevated lactate, and oliguria consistent with TLS. Hematology-oncology was consulted and expressed concern for high-grade neuroendocrine tumor or lymphoma. She was managed with aggressive intravenous hydration, loop diuretics, and corticosteroids. Despite these efforts, urine output was insufficient to manage the metabolic derangements. The patient became hypotensive, tachypneic, and required supplemental oxygen, prompting transfer to the intensive care unit for vasopressor support and initiation of continuous renal replacement therapy. Despite aggressive management, she progressed to refractory shock. In light of her poor prognosis and rapidly deteriorating condition, goals of care discussions were held with the family, and she was transitioned to comfort-focused care, and died shortly after. Final pathology from the liver biopsy resulted after the patient passed away and revealed a high-grade carcinoma with extensive necrosis. Immunohistochemistry findings were most consistent with a poorly differentiated squamous cell carcinoma of the lung.
Discussion: sTLS is rarely reported in solid tumors and is exceptionally uncommon in squamous cell carcinoma of the lung. Risk factors for poor prognosis in sTLS in solid tumors include bulky metastatic disease (especially with hepatic involvement), elevated LDH, rapid proliferation, and extensive tumor necrosis, all of which were present in this case [2]. Unlike chemotherapy-associated TLS, sTLS may present insidiously and progress rapidly, making early recognition challenging.
Conclusions: This case highlights the importance of maintaining a high index of suspicion for TLS in patients with large, aggressive, untreated solid tumors, as timely identification and intervention may be lifesaving.