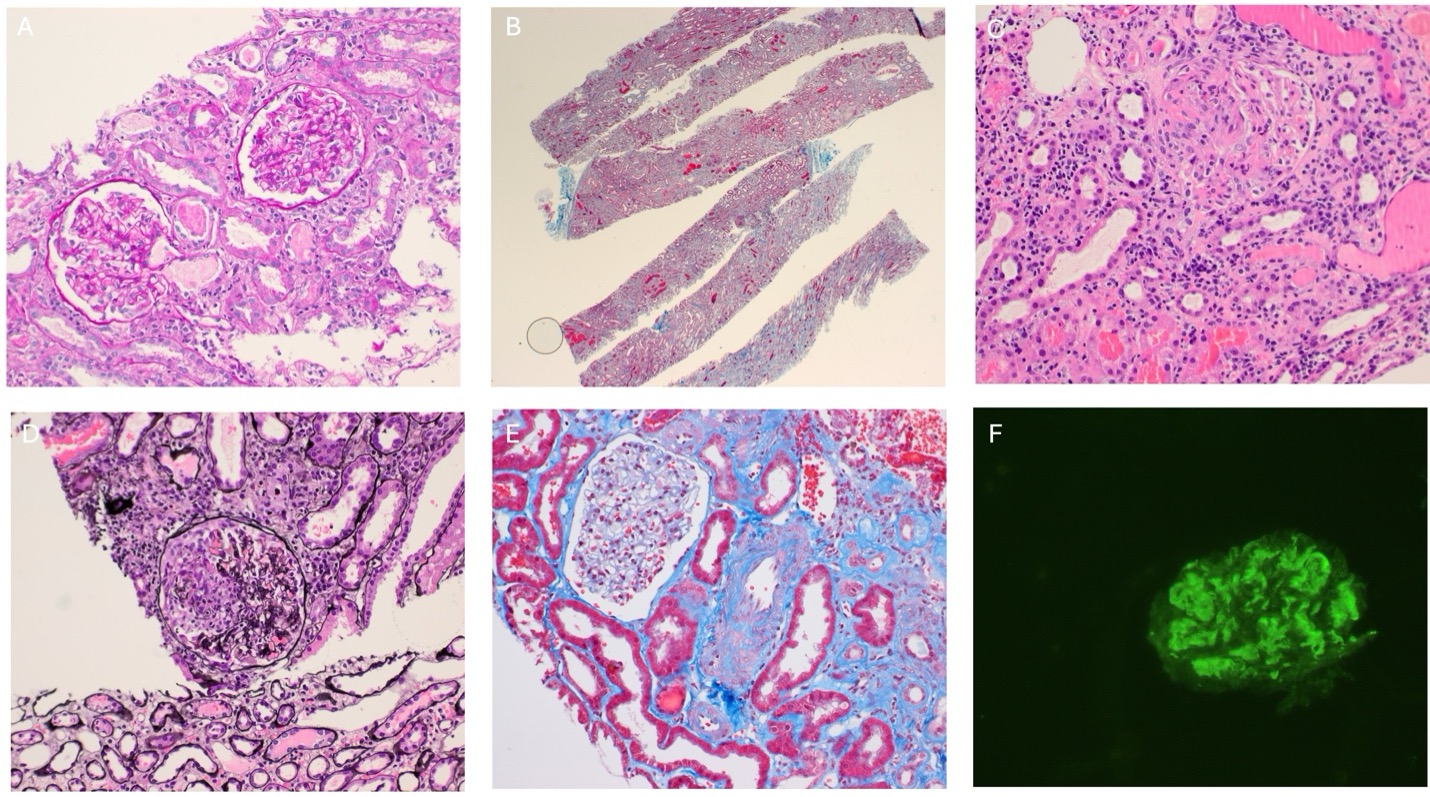
Case Presentation: A 42-year-old man with untreated chronic hepatitis C and a history of culture-negative endocarditis status post porcine aortic valve replacement presented with six months of progressive fatigue, weight loss, fevers, pancytopenia, renal dysfunction, splenomegaly, and a macular rash. Imaging revealed massive splenomegaly, ascites, and lymphadenopathy. Renal biopsy showed diffuse crescentic glomerulonephritis with C3-dominant immune-complex deposition. Serology demonstrated strongly positive Bartonella henselae and Bartonella quintana IgG titers, positive Bartonella PCR, and typhus-group IgG positivity. Echocardiography showed no vegetations, but the findings met 2023 Duke–ISCVID criteria for definite culture-negative endocarditis. The patient improved with doxycycline, rifampin, and corticosteroids, relapsed after prematurely discontinuing therapy, and improved again after treatment was reinitiated.
Discussion: This case illustrates the interplay of multiple concurrent infectious and immune-mediated processes. Bartonella infection is known to cause immune-complex glomerulonephritis and cryoglobulinemia, but the patient’s untreated hepatitis C is also a well-recognized driver of mixed cryoglobulinemia. Both infections likely contributed to his immunologic abnormalities, and their relative contributions cannot be fully separated. Strong seroreactivity to both B. henselae and B. quintana, along with positive typhus-group serology, highlights the challenges of serologic cross-reactivity and raises the possibility of alternative transmission routes such as body-louse exposure rather than cat contact alone. Because the Bartonella PCR used detects DNA at the genus level but does not differentiate species, the true etiologic species remains uncertain. Despite negative echocardiography, the combination of high-titer serology, PCR positivity, prosthetic valve, and systemic immune phenomena supported a diagnosis of definite culture-negative endocarditis under updated Duke–ISCVID criteria
Conclusions: Bartonella infection should be considered in patients with systemic illness, culture-negative endocarditis, and glomerulonephritis, even when echocardiography is unrevealing. Interpretation of cryoglobulinemia and immune-complex disease requires caution when multiple potential drivers, such as hepatitis C and Bartonella, are present. Cross-reactive serologies and species-nonspecific PCR findings emphasize the need for careful clinical interpretation. Early recognition, prolonged combination antimicrobial therapy, and judicious use of corticosteroids remain central to favorable outcomes.
.jpg)