Case Presentation: A 3-year-old girl with history of recurrent otitis presented with 2 weeks of gait instability. Her family reported sudden onset of ataxic gait, requiring assistance with balance while ambulating. She had a preceding illness with congestion and dry cough for which she was started on a 10-day course of Amoxicillin by her primary doctor. She was only on cetirizine at admission. Her vital signs were within normal limits. She was well appearing, though fussy. She had absent reflexes in her lower extremities and inability to stand from sitting. She had a broad-based gait, but normal sensation and coordination for age. Her strength was intact in the upper extremities. Initial laboratory testing, including CBC, electrolytes, liver function tests, inflammatory markers, and urinalysis was unremarkable. Outside hospital imaging, including CT head and plain radiographs of the bilateral hips and lower extremities, was normal. MRI brain was normal; however MRI spine revealed diffuse enhancement of the spinal cord nerve roots, most notable in the cauda equina. Lumbar puncture demonstrated albuminocytologic dissociation (Table 1). She was diagnosed with GBS and treated with 3 days of IVIG. Her symptoms improved and she was standing and walking independently at 1-week follow up.
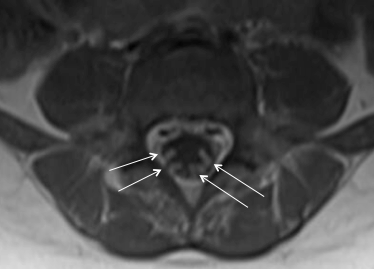
Discussion: Guillain-Barré syndrome is an acute polyradiculoneuropathy typically characterized by symmetric ascending paralysis. It is thought to be due to an inflammatory demyelination of neurons following infection or immunization, but may be idiopathic as well. While older children and adults classically present with ascending weakness, paresthesias, and flaccid paralysis, this is often not the case in younger patients, who are more likely to present with ataxia or abnormal gait. In our case, the initial symptoms were simply gait and balance disturbance and there was relatively little progression over two weeks after the onset of symptoms. This subtle and atypical presentation can make the diagnosis more challenging. GBS is a diagnosis based on clinical presentation, but is supported by other findings, including absent reflexes, albuminocytologic dissociation in the CSF and enhancement of spinal nerve roots with contrast-enhanced MRI (Figure 1). While GBS is less common in children than adults (0.34–1.34 per 100,000 per year in children compared to an estimated 1.1-1.8 in adults), the general pediatrician should consider this diagnosis in young children with gait disturbance and a negative musculoskeletal workup. Early treatment with IVIG or plasma exchange can shorten recovery time in these patients.
Conclusions: General pediatricians should be aware of differing presentations of Guillan-Barré syndrome, which include gait abnormalities in younger children.