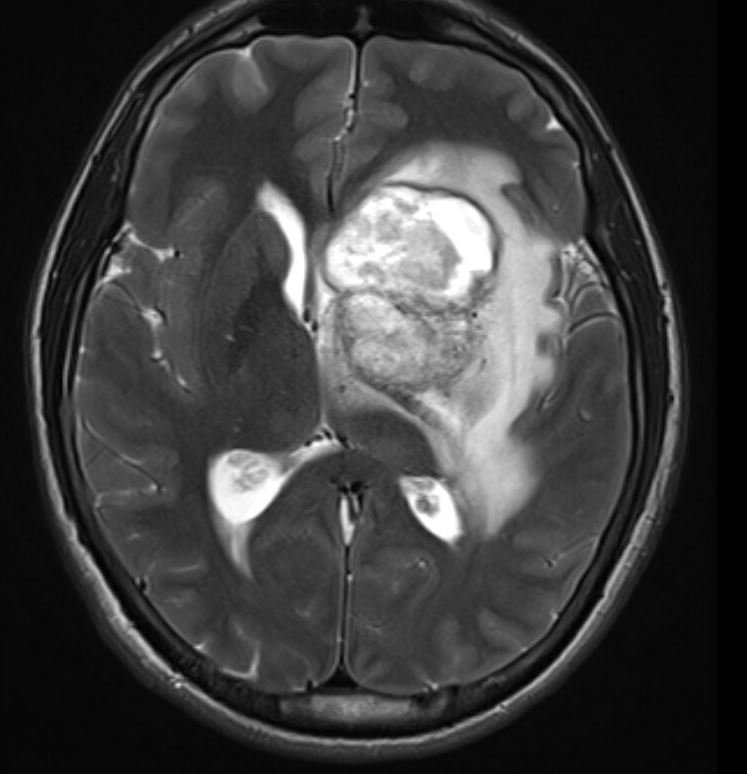
Case Presentation: A 21 year-old male with history of untreated Hepatitis C and intravenous drug use presented with acute right-sided weakness, fevers and altered mental status. Exam was significant for word-finding difficulty, asymmetric pupils, and 4/5 right-sided upper extremity and facial weakness. Labs were remarkable for leukocytosis. Brain MRI demonstrated expansile process involving the left basal ganglia, internal capsule, thalamus with hemorrhagic changes and surrounding edema. Lumbar puncture did not yield organism isolates. Blood cultures, EEG, echocardiogram and panorex were unremarkable. Serologies were negative for HIV, EBV, hepatitis B, histoplasma, blastomycosis, cryptococcus, coccidioides, aspergillus, toxoplasma and syphilis. Neurosurgical stereotactic biopsy obtained on hospital-day (HD) 5 revealed histopathologic findings diagnostic for rhizopus oryzae. Otolaryngologic evaluation demonstrated no rhino-oral involvement. His disease was deemed not amenable to neurosurgical resection, and liposomal amphotericin B and posaconazole were initiated. Evaluation for immunodeficiency was negative and hemoglobin A1C was 5.2. After initial improvement he progressively declined over the following two weeks with progression of mass effect on imaging. Neurosurgery intervened on HD 19 with placement of intracavitary drain. Posaconazole was replaced with planned course of caspofungin in addition to amphotericin. The patient was ultimately discharged with guarded prognosis. Remarkably, assessment eight weeks post-discharge demonstrated clinical improvement and disease regression on brain MRI.
Discussion: Zygomycosis is classically associated with diabetic ketoacidosis and immunosuppressed states and confers a high mortality. Isolated cerebral zygomycosis in immunocompetent patients associated with intravenous drug use confers an even higher mortality rate (80%). A recent publication that examined 929 reported cases of zygomycosis since 1885 demonstrated only two cases associated with IVDU prior to 1980 but nearly forty cases in the decades after. 20 of 22 reported cases of cerebral mucor demonstrated basal ganglia involvement and 62% of all zygomycoses associated with IVDU is isolated to the cerebrum providing an important diagnostic clue. Blood vessel thrombosis and resulting tissue necrosis leads to poor penetration of antifungal agents, therefore, even in non-surgically resectable disease, debridement of necrotic tissues may decrease disease burden and increase the odds of survival. Additionally, rhizopus oryzae express the target enzyme for echinocandins and survival advantage of combination amphotericin and caspofungin compared to amphotericin alone has been demonstrated in both preclinical and a retrospective cohort study (80% v. 18%). It is critical that hospitalists maintain a high index of suspicion as initiation of antifungals within 5 days after diagnosis of mucormycosis is associated with improvement in survival (83% vs. 49%).
Conclusions: The incidence of isolated cerebral zygomycosis in immunocompetent patients is rising as the prevalence of intravenous drug use increases. The management of these patients remains largely unknown and understudied. Surgical debridement and amphotericin are the mainstays of current therapy, however, caspofungin is a potential adjuvant. Ultimately, successful treatment of zygomycosis is reliant on a combination of early diagnosis, surgical debridement and adequate antifungal therapy.