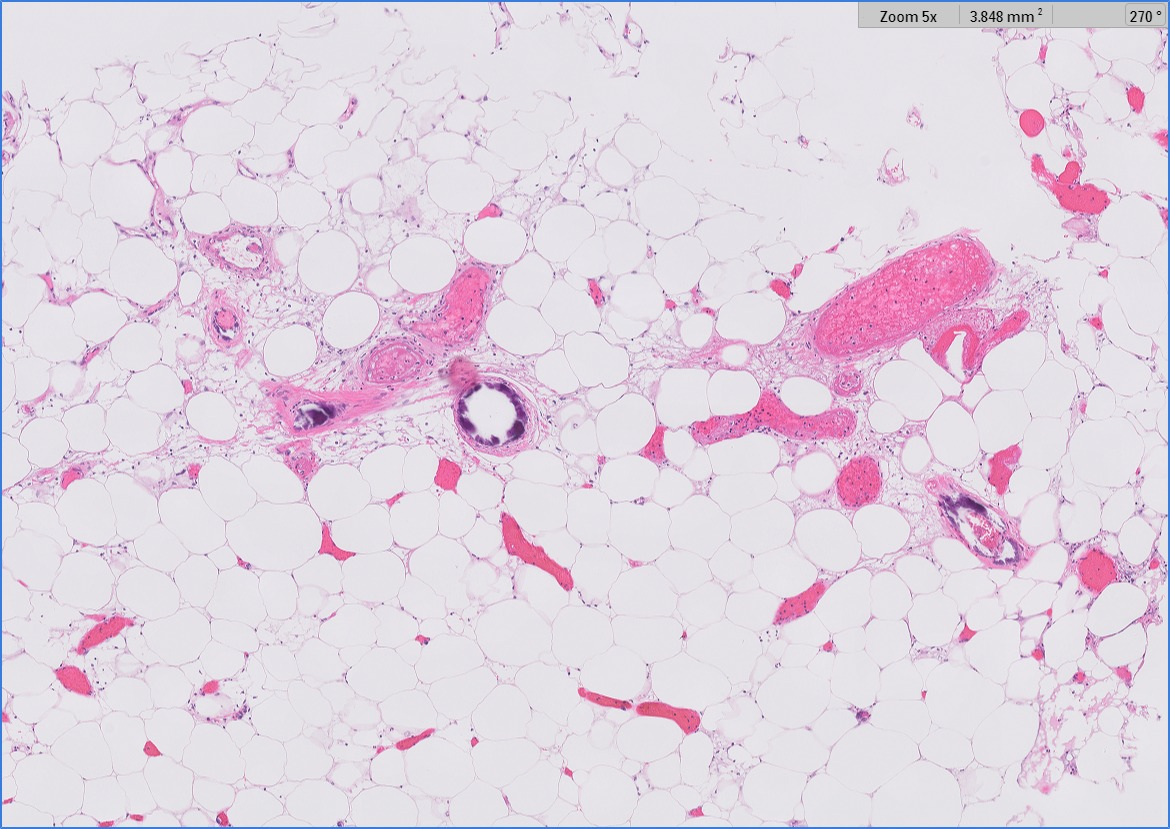
Case Presentation: A 47-year-old woman with obesity, diabetes mellitus, hypertension, and liver cirrhosis presented with septic shock and acute renal failure along with volume overload necessitating urgent dialysis. She received broad-spectrum antibiotics, which were later narrowed to cover extended spectrum beta-lactamase-producing (ESBL) Enterobacter found in her blood cultures. Fifteen days after admission and initiation of hemodialysis, she developed an erythematous rash on her left medial thigh presumed to be cellulitis. Morbid obesity and extremely large pannus limited daily exams. The rash persisted despite courses of Doxycycline and Ertapenem. CT scan of the left thigh revealed extensive soft tissue edema without an underlying abscess. In light of intermittent fevers, myalgias, and joint pains, an extensive rheumatologic workup (ANA, RF, ANCA, cryoglobulins, and anti-phospholipid markers) was performed, which was unrevealing. Subsequently, a painful ulcer with a necrotic border appeared at the site of the rash, progressing to multiple small ulcers. Two weeks after the initial appearance of the rash, a skin biopsy confirmed the diagnosis of calciphylaxis. Treatment with sodium thiosulfate and cilostazol along with diligent wound care was initiated, with a plan to reassess if inadequate improvement in three months.
Discussion: Calciphylaxis is a rare and lethal condition of skin ischemia and necrosis secondary to calcium deposition in dermal and hypodermal arterioles and capillaries [1]. Reduced blood flow leads to extremely painful lesions that are highly prone to infection. The disease, frequently associated with end-stage renal disease (ESRD) and dialysis, carries an approximately 40% mortality rate at six months [2,3]. Calciphylaxis is often initially misdiagnosed, most commonly as cellulitis [4]. The variable appearance of the lesions and their propensity to affect areas of the body with high adiposity, which may be difficult to visualize, make it challenging to identify [5]. However, incidence of calciphylaxis appears to be increasing, and earlier consideration of the disease will allow for more rapid initiation of appropriate treatment and precautions [6]. Early contact precautions and wound care, in particular, are essential for preventing infection, which is the primary cause of mortality from calciphylaxis [7]. Additionally, this case highlights the ways in which better recognition of non-infectious skin pathologies such as calciphylaxis can improve our antibiotic stewardship. Our patient received a number of broad-spectrum antibiotics before an alternative diagnosis was made, and earlier detection of her calciphylaxis could have limited her exposure to these agents. Finally, this case is an excellent example of integration among many different medical subspecialties. A coordinated effort from multiple subspecialties allowed an accurate diagnosis and implementation of disease-directed management.
Conclusions: A non-healing rash has a broad differential including many potential infectious causes. Less common conditions such as calciphylaxis should be considered as well, particularly in patients with renal disease requiring dialysis. Increased awareness and earlier recognition of calciphylaxis will allow for earlier implementation of infection precautions and appropriate treatment, as well as promote antibiotic stewardship.